")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Planning for Hospital Discharge for Older Adults in Uganda: A Qualitative Study Among Healthcare Providers Using the COM-B Framework
Authors Owokuhaisa J, Schwartz JI , Wiens MO, Musinguzi P, Rukundo GZ
Received 13 July 2023
Accepted for publication 22 October 2023
Published 2 November 2023 Volume 2023:16 Pages 3235—3248
DOI https://doi.org/10.2147/JMDH.S430489
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Judith Owokuhaisa,1 Jeremy I Schwartz,2,3 Matthew O Wiens,4,5 Pius Musinguzi,6 Godfrey Zari Rukundo7
1Faculty of Medicine, Department of Physiotherapy, Mbarara University of Science and Technology, Mbarara, Uganda; 2Uganda Initiative for Integrated Management of Non-Communicable Diseases, Kampala, Uganda; 3Section of General Internal Medicine, Yale University School of Medicine, New Haven, CT, USA; 4Institute for Global Health, British Colombia Children’s Hospital, Vancouver, British Columbia, Canada; 5Department of Anaesthesiology, Pharmacology and Therapeutics, University of British Columbia, Vancouver, British Columbia, Canada; 6Department of Nursing, Faculty of Medicine, Mbarara University of Science and Technology, Mbarara, Uganda; 7Department of Psychiatry, Faculty of Medicine, Mbarara University of Science and Technology, Mbarara, Uganda
Correspondence: Judith Owokuhaisa, Email [email protected]
Background: Proper discharge planning enhances continuity of patient care, reduces readmissions, and ensures safe and timely transition from health facility to home-based care. The current study aimed at exploring the healthcare providers’ perspectives of discharge planning among older adults, with respect to barriers and facilitators within the Ugandan health system.
Methods: We conducted a qualitative exploratory study that used one-on-one interviews (Additional file 1) to describe individual perspectives of healthcare providers in their routine clinical care setting. The study included medical doctors (including consultants and physicians), nurses and physiotherapists directly involved in providing care to older adults. We conducted 25 in-depth interviews among healthcare providers for older adults with non-communicable diseases. The audio-recorded interviews were transcribed verbatim. Data were manually organized using a framework matrix guided by the COM-B domains (capability, opportunity and motivation) as the broad themes and sub-themes (physical and psychological capability, social and physical opportunity, reflective and automatic motivation) that influence behavior change (discharge planning).
Results: Discharge planning was facilitated by availability of discharge forms, continuous medical education and working experience. The barriers to discharge planning were understaffing, workload/insufficient time, lack of discharge planning guidelines, lack of multidisciplinary approach and congested inpatient wards. Both barriers and facilitators were at various levels of healthcare service delivery such as patient, caregiver, healthcare provider, health facility and policy levels.
Conclusion: Barriers to discharge planning spread across all levels of healthcare service delivery, but they can be addressed by enhancing the facilitators. This calls for a multi-level action to ensure adequate and quality patient care during and after hospitalization.
Keywords: discharge planning, barriers, facilitators, COM-B framework
Background
Improved healthcare systems and increased survival increased the aging population and health implications associated with aging have become a global population concern of the 21st century. Older adults defined by the United Nations as persons older than 60 years1 contribute to contribute 11% of the global population and are expected to increase to 20% by 2050.2 In 2019, the global life expectancy was estimated at 72 years: 74.2 years for females and 69.8 years for males (WHO, 2019). The global population of older adults in 2017 was estimated at 962 million and was projected to reach about 2.1 billion by 2050 health, and two-thirds are in developing countries. The global population of older people in sub-Saharan Africa is 5% (43 million) which is expected to increase even higher by 2030. In Uganda, older people contribute 2.7% of the entire population and life expectancy has increased from 50 to 63 years over the past ten years.
Aging comes with both medical and social challenges which require appropriate and timely interventions. Unquestionably, studies have revealed that older adults contribute to up to 23% of the total global burden of diseases.3 Literature from the global north shows that older adults are hospitalized more frequently and for a longer period of time than any other age groups. This is attributed to such age groups tending to suffer more severe forms of diseases that are difficult to diagnose and treat.4
A successful discharge from acute care settings to the community requires coordination and communication between the healthcare workers and between the healthcare team and patients themselves. This transition of care represents one of the most vulnerable periods during an illness. Indeed, one-third of hospitalized older adults encounter more complications post-discharge, including reduced functional capacity, than at admission.5 More so, about 5% of the older adults die during hospital admission and 20–30% pass on within one year after hospital discharge.4 Postdischarge deaths often times are more than in-hospital deaths. In addition, majority of post-discharge deaths occur at home, suggesting that the point of discharge represents an opportunity for innovative interventions to improve health outcomes among older adults.
A high quality of care at the facility necessitates patient-centered discharge planning. Depending on the individual needs of the patient, effective discharge planning supports the continuity of health care between the healthcare setting and the community; it is described as “the critical link between treatment received in hospital by the patient, and post-discharge care provided in the community.6” The purpose of discharge planning is to ensure continuity of quality care between the hospital and the community. In addition, discharge planning aims to reduce medical costs, improve patient outcomes, reduce length of stay and improve post-discharge recovery.7 The process aims at ensuring that patients are discharged at an appropriate time and that sufficient support is accessible in the community when needed.7 During the discharge planning process, certain parameters are put into consideration and these include the following: (1) early identification and assessment of patients requiring assistance with planning for discharge; (2) Patient, family, and health-care team collaboration to facilitate discharge planning; (3) recommending options for the continuing care of the patient and referring to accommodations, programs, or services that meet the patient’s needs and preferences; (4) liaising with community support groups and care facilities to promote patient access and to address gaps in service; and (5) providing support and counseling to patients and families during hospitalization.
Discharge planning has diverse classifications by different scholars. McGeehan and Coulton (1985), classified discharge planning into (1) informal discharge planning and (2) formal discharge planning.8 Informal discharge planning is where the discharge planning was done by the attending doctor and the primary nurse without following any discharge planning procedures and guidelines, without any communication between the hospital and the community, and without any discharge planning record. This is the commonest discharge planning in sub-Saharan Africa Uganda inclusive. While in informal discharge planning, the patient and the family participate in the discharge planning process, and there are well-organized discharge planning procedures and guidelines, good communication between the hospital and the community, and a detailed discharge planning record.
However, in 1990, Debra and Leah used different terms for informal and formal discharge planning: (1) ordinary discharge planning and (2) specialized discharge planning.9 Ordinary (“informal” or “usual”) discharge planning is provided by the attending physician and nurses of the inpatient unit. In specialized (“formal” or “interdisciplinary”) discharge planning, the hospital’s discharge planning staff includes a social worker or a registered nurse of the social work department.
Several institutions worldwide have adopted discharge planning and integrated it into national practices. In the global North, discharge planning is standard of care, but the global South is largely neglecting it.10 Some evidence exists from sub-Saharan Africa, but it is focused on children, but not yet any focusing on older adults, though some findings might be relevant across the lifespan. Studies conducted in Uganda focusing on children have shown improved outcomes after discharge through an educational intervention and community level referrals for follow-up.11 Discharge planning education and follow-up after discharge appear to be essential components needed to improve the long-term survival of older adults admitted especially with serious illness. To address this evidenced gap in post-discharge care for older adults in sub-Saharan Africa, we conducted this study to explore the healthcare providers’ perspectives of discharge planning among older adults, with respect to barriers and facilitators within the Ugandan health system.
Theoretical Framework
This study was built on a theoretical model of behavior change. The Capability, Opportunity, Motivation, Behavior (COM-B) model is a theory of behavior change ideally suited to contribute to an improved understanding of discharge planning behavior among health workers.12 The COM-B model employs several distinct explanatory components to understand behavior adoption or change. For behavior change to take place, there should be interactions between one or more of the capabilities (physical and psychological) to carry out a behavior, opportunities (physical and social) and motivation (reflective and automatic) to perform a desired behavior.12
We characterized Capability as physical (skills, abilities, proficiencies) and psychological (knowledge, memory, behavioral regulation) abilities needed by health workers to carry out discharge planning; Opportunity as social (peer pressure, norms, conformity, and comparisons) and physical (environmental context and resources) influences to discharge planning; and Motivation as reflective (beliefs about capabilities, roles, intentions), and automatic (emotions, reinforcements such as incentives or punishment).
Methods
Study Design and Setting
We conducted a qualitative exploratory study that used one-on-one interviews to describe individual perspectives of healthcare providers in their routine clinical care setting. Our aim was to identify barriers and facilitators to discharge planning among older adults by health workers at Mbarara Regional Referral Hospital (MRRH) in southwestern Uganda. The qualitative interviews were guided by the COM-B framework.13 We carried out this study from an exploratory perspective using a participant-oriented perspective for improved engagement, acceptability, and clinical outcomes. The study was designed by JO in consultation with GZR, JIS and MOW.
The study was carried out at internal medicine department of MRRH, southwestern Uganda. MRRH is a public referral health facility and the teaching hospital of the Medical School of Mbarara University of Science and Technology (MUST). The hospital serves a population of over four million people in its catchment area. MRRH is located 270 Km from Kampala in southwestern Uganda. The internal medicine department admits cases with both communicable and non-communicable diseases. It admits about 50 older adults per month. The department is run by a team of 10 consultants, 8 nurses, 1 clinical officer, 1 pharmacist, and residents.
Study Participants
The study participants included medical doctors (including consultants and physicians), nurses (general practitioners and registered) and physiotherapists directly involved in providing care to old adults at the inpatient department of internal medicine at MRRH. JO recruited study participants purposively through phone calls to schedule in-person interviews. Nine potential participants declined to participate, one was not interested in the study, six failed to get time to participate, and another had travelled abroad. The study purpose was introduced to the targeted participants and only those who provided written informed consent were included in the study.
Data Collection Tool
We developed a semi-structured interview guide (Additional file 1) corresponding to the COM-B domains as the a priori themes with questions tailored to the practice of discharge planning. The study tool was pretested, and the responses from the pre-test were used to amend the guiding questions.
Data Collection Procedure
Data was collected between May and June, 2022. In-depth interviews were conducted by a research assistant with a public health background and experience in conducting qualitative research interviews. The participants were informed about the purpose of the study, namely to gain their perceptions about factors influencing their practice in discharge planning among older adults with admitted. All participants were assured about confidentiality of their responses and that any publications would be de-identified with respect to quotations from the interviews.14 Informed consent was obtained, and interviews were conducted from the participants’ offices. Written consent was obtained to audio record the interviews, supported with field notes. During the interviews, open-ended questions were sequentially asked following the interview guide. Probes were used to either obtain more information or for further clarification. All interviews were conducted in-person, in English language (the official language in Uganda), and lasted for approximately 30 to 60 minutes. After the interview, each participant was given 30,000 Ugandan shillings (equivalent to 8 US Dollars) as an incentive.
Data Management and Analysis
All audio recorded interviews were transcribed verbatim by the research assistant, and the transcripts reviewed by JO for accuracy,15 inserting notations for pauses, clarification of information and punctuations. All the transcripts were read and re-read by JO and PM together with other two research assistants to familiarize with the data and the overall meaning.16 Data were manually organized using a framework matrix17 guided by the COM-B domains (capability, opportunity and motivation) as the broad themes. The rows were used for sub-themes (physical and psychological capability, social and physical opportunity; reflective and automatic motivation), while the columns represented the subgroups (from probes, field notes), and responses from the participants.16 The content in the cells of the raw matrix was mapped to the COM-B domains to check that the responses were correctly placed under each category.17 Coding was done by PM and research assistants independently and reviewed by JO, JIS and MOW for consistency checks to ensure rigor.18,19 Where there was disagreement on content mapping, there was discussion and responses switched to where they were most fitting by consensus.
Results
Participant Demographic Characteristics
A total of 25 participants were recruited into this study. Most of the participants were male (64%), 40% were aged between 25 and 35 (40%) years. Just over half of the participants were doctors (56%), followed by nurses (28%) and physiotherapists (16%). Forty-four percent of the participants had a working experience of 6–10 years with only 4% having more than 20 years of experience (Table 1).
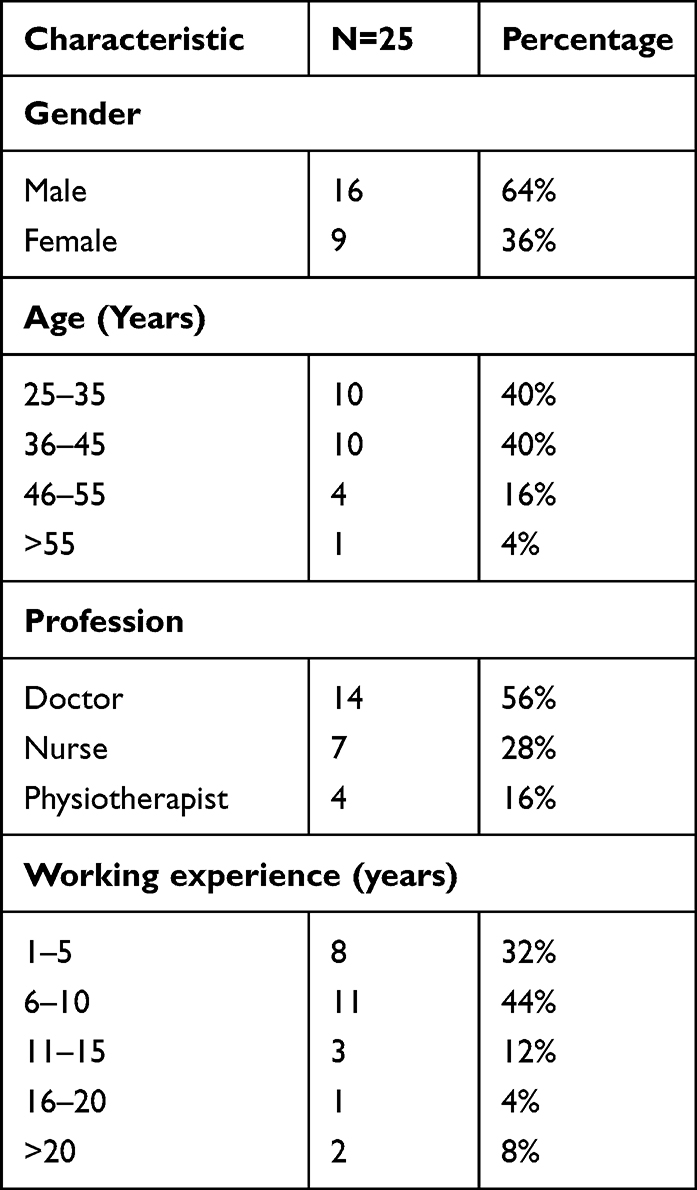 |
Table 1 Demographic Characteristics |
Barriers and Facilitators to Discharge Planning
The results were organized corresponding to three COM-B domains that guided the interview including i) Capability – physical and psychological; ii) Opportunity – physical and social; and iii) Motivation – reflective and automatic (Additional file 2). The factors that negatively affected the components of the COM-B framework were categorized as barriers (Table 2) and those that positively affected the components were grouped as facilitators (Table 3).
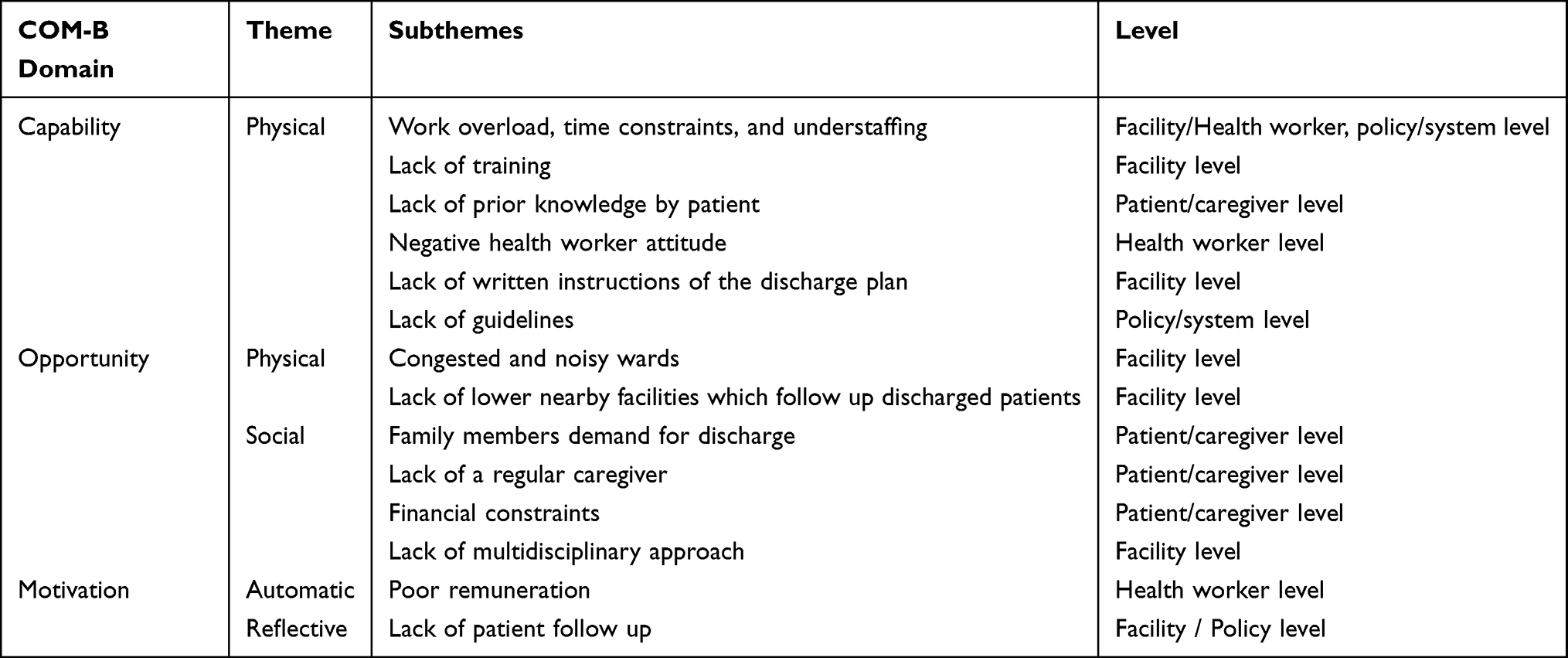 |
Table 2 Barriers to Discharge Planning Mapped Onto the COM-B Model |
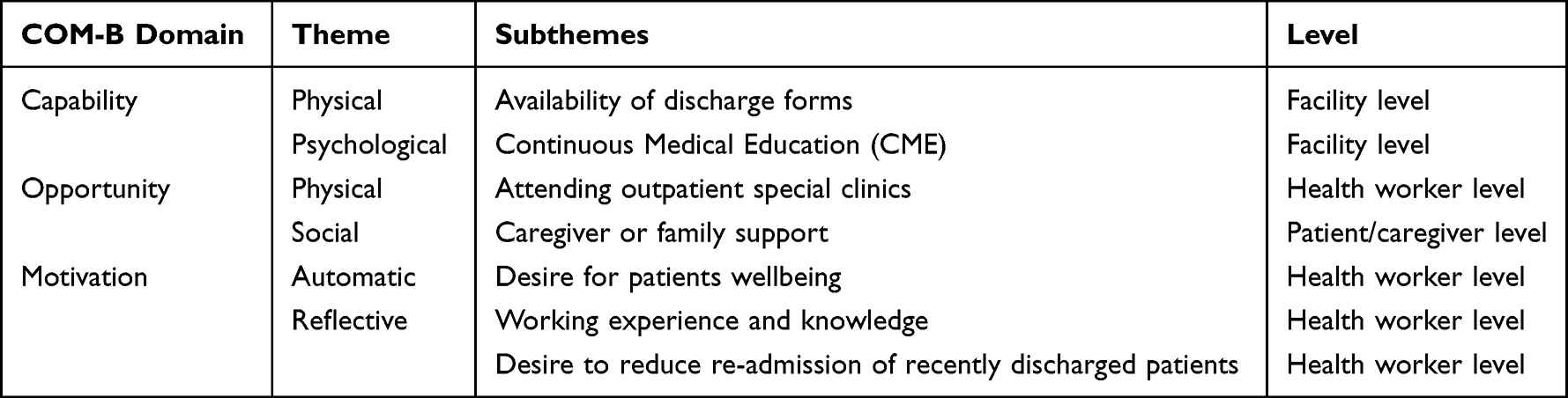 |
Table 3 Facilitators of Discharge Planning Mapped Onto the COM-B Model |
Domain 1: Capability
Barriers
The barriers of discharge planning were described under each of the subcategories of the COM-B model that is physical capability, psychological capability, physical opportunity, social opportunity, automatic motivation and reflective motivation.
Physical Capability
Multiple Responsibilities/ Work Overload/ Understaffing
Most participants described that they had many responsibilities to perform. As a result, they lacked sufficient time to perform a detailed discharge plan. Some participants said that they were both university and hospital staff and thus had multiple responsibilities to fulfil. In addition, participants said that they could not find time to sit with the patient and caregiver to make a proper and detailed discharge plan. One of the participants mentioned that they end up giving very sketchy information which may not adequately address the patients’ healthcare needs after discharge from hospital to their homes. Furthermore, most of the participants attributed this to understaffing, noting that the health worker to patient ratio was unfavourable given that discharge planning required much time.
…you have also other responsibilities surrounding you so you have to teach your students and remember most of the hospital staff, they are university staff. The hospital doesn’t have enough staff especially doctors. So the time you’re going to give to the patient at the discharge is not going to be enough. (Doctor, 34 years male)
Psychological Capability
Insufficient Knowledge and Skills
Some participants mentioned that they lacked knowledge and the skills to facilitate the discharge process due to a difference in knowledge and expertise concerning discharge planning. One of the participants further described that there was a knowledge gap which needed to be bridged.
This is a teaching hospital that has junior and senior doctors. So sometimes there is a difference in knowledge and some people let me say an intern or a student because he’s on ward and you find he’s the one discharging a patient…and then you find the next day the patient comes back. So there are those knowledge differences…. (Doctor, 47 years female)
Family Members Demand for Discharge
Some participants reported that at times, the discharge planning process was disrupted by family members who demanded for discharge of their patients even against medical advice. Family members demanded for unplanned discharge because of lost hope that their patient had failed to improve or even they were afraid of the uncertainties. In such instances, proper discharge planning was not done.
… off course there are some people who insist and say no, me I want to go home whatever the case is. Some of them are because they are impatient, some of them are because they see their patient is probably about to die and they say, he would rather die from home. It is going to be expensive transporting the body. We discharge and we call it discharge against medical advice. (Doctor, 45 years male)
Negative Health Worker Attitude
One of the participants said that some health workers took it for granted that patients already knew enough about the disease conditions and ended up not taking them through the proper discharge process.
…some of us have negative attitude you’re like, he has been a diabetic patient, why bother to go into those details? Forgetting that sometimes they forget because it has taken long…Or they picked it wrongly, you don’t go out to see…to get a demonstration whether they understood what you wanted…So I may attribute that one to negative attitude. (Nurse, 47 years female)
Lack of Written Instructions of the Discharge Plan
Some participants said that the discharge plan was not often documented by health workers. There were no written instructions given to the patients and the caregiver for future reference after going home. This left the patients and the caregivers without any material reference in case they forgot the instructions given to them after reaching home.
…now you’re telling them [patient/caregiver], not documenting and therefore you think they are documenting in the head? This can easily be forgotten by the time they [patient and caregiver] reach home. But when it is written [discharge plan] when they reach home even if they don’t know how to read, they can get somebody who can read to them. (Nurse, 36 years male)
Low Level of Understanding of Patient/Caregiver
Some participants noted that some patients and caregivers were illiterate, hence unable to clearly understand the information given to them at discharge. This made it hard for them to follow the instructions in the discharge plan.
…ignorance is also a factor. I mean, not all patients are learned patients. And it may not be a guarantee you may communicate but the way information is perceived may be totally different because our understanding is totally different. (Nurse, 28 years male)
Facilitators
Physical Capability :Availability of Discharge Forms
Some participants noted that there was a discharge form which guided health workers to capture the necessary information about the patient. It identifies the patient’s information including the disease condition and the care he/she has received from the hospital. One of the participants added that this information was then used to make a discharge plan.
So, in the discharge planning…you know there is a discharge form which captures a patient’s name, age occupation, place of residence and then the diagnosis of the patient and then you write the summary of the patient’s conditions; what brought the patient to the hospital and then what you have given the patient … and what you have done to the patient in terms of investigations and then after that you make the (discharge) plan…. (Doctor, 34 years male)
Psychological Capability
Continuous Medical Education (CME)
Some participants revealed that having regular CME helped them to acquire current knowledge, thus capacitating them to do proper discharge planning. Another participant added that in CME, junior health workers get an opportunity to be guided by the senior health providers on issues regarding patient care and discharge.
Of course, for the knowledge gap we have serial (Continuous medical education) CMEs and I hope they go on. And also, continuous education even during working hours most especially when we meet someone on these stations where many senior doctors have always been talking to the junior doctors regarding when and how to discharge a patient who is admitted with what disease, how long they should be in hospital. Yeah, that one is always on going. (Doctor, 47 years female)
Domain 2: Opportunity
Barriers
Physical Opportunity
Lack of Discharge Policy or Guidelines
Most of the participants reported that they lacked clear guidelines on discharge planning and that disrupted the process. One participant mentioned that he had to first look for the information to include in the discharge plan which took him more time.
I may say I have not seen any policy or guidelines on how to discharge a patient. I haven’t seen it anywhere; I don’t know whether it’s there or not. So, I think also the ministry has to give us the guidelines on how to discharge such kinds of patients and what they should do, other than looking here and there to get the information…because the facility has not put guidelines for us to follow. (Nurse, 47 years female)
Lack of a Private Environment for Discharge
The participants stated that they lacked a private environment where discharge process could be effectively done. Some participants mentioned that discharge is done in the general wards which are congested and noisy. One participant described such an environment as not conducive for a health worker to deliver an effective discharge plan. In addition to that, the participant expressed concerns about the patients’ privacy since the discharge plan might involve sharing sensitive information about the patient.
… discharge plan I would think it wouldn’t be best done in ward, it would be best done somewhere in an isolated room where you’re seated on a chair with a patient which is not here. It’s good in the private setting where you know you have a room and you’re sharing this information in a calm place with the caregiver, there is no noise left and right. So also privacy is a point to talk about. We may not be so…but a conducive environment is also something that is supposed to be looked at. (Nurse, 28 years male)
Lack of Follow-Up Care in Lower Nearby Facilities
The participant revealed that there was no down ward referral which affected the post-discharge care. Lack of a clear strategy about down ward referral increased the burden on them because patients kept coming back to the health facility.
Ideally in Uganda we don’t have a program that does down ward referrals and it’s a challenge because you can’t send someone to a lower health facility. We have been sending people to the nearby health centres but eventually they don’t find care there and they have to come back. (Doctor, 29 years female)
Social Opportunity
Lack of a Consistent Caregiver
Some participants revealed that some patients lacked social support from caregivers who are the preferred recipients of the information given by health workers at the time of discharge. Another participant explained that sometimes the caregivers of the same patient were not consistent, they kept on changing. This was reported to be a disruption to the discharge plan because the health worker gave bits of information about patient care after discharge to different caregivers thus making the implementation of the discharge plan difficult.
Even the older people usually don’t have stable caregivers. Today there is another caregiver you teach; on discharge you encounter a new caregiver who doesn’t know that the patient is even diabetic. So you have to again go back to square zero. (Nurse, 36 years male)
Financial Constraints
Most participants believed that discharge planning was hindered by the financial situation of many patients and their families. For instance, one of the participants explained during discharge, the patient and family were always given a list of medication to buy for use while at home. This drifted the attention of the patient and the caregiver to how to raise the money to buy the medication rather than listening to the instructions being given to them regarding patient care at home.
Of course, these patients also have issues, financially you find that you’re trying to tell someone about certain information but their mind is divided because of financial constraints. So sometimes they cannot sit and focus and listen at what you’re talking about. So you find that you’re telling someone you’re going to buy, you’re going to buy; so someone is already having stress of ‘you’re going to buy before they even listen to the information you’re going to give them. So that can also hinder or influence a better discharge plan because you can give that information but they are not taking it up. (Nurse, 28 years male)
Lack of Interdisciplinary Approach
Most participants admitted that different cadres worked in isolation yet managing the same patient. They revealed lack of multi-disciplinary approach to discharge planning as a major setback to the whole process. As a result of this, the patient and caregivers end up receiving an incomplete discharge package without the input of some healthcare professionals.
The other one is we also don’t have um…multi-disciplinary team approach on a patient management. We don’t usually work as a team. We have the different cadres around, we have physiotherapists, we have nurses, we have pharmacists but we do not work as a team. (Doctor, 37 years male)
Facilitators
Physical Opportunity: Attending Outpatient Special Clinics
Some participants explained that, however, much time may not be adequate for a proper discharge from ward, and the outpatient specialized clinics offered better opportunity for proper planning. One participant said that these clinics were attended by fewer patients on a daily basis who got a one-on-one interaction with the senior health workers.
We get better times when we are in the outpatient specialized clinics with the patients, as seniors, as consultants… That gives me enough of the time even to interact with the patient directly and talk to them individually…. (Doctor, 34 years male)
Social Opportunity
Caregiver or Family Support
Most participants described that the patients’ family and caregivers were part and parcel of the whole discharge process. Some participants reported that the home care instructions were often given to the caregivers since the patients were old, sometimes cognitively impaired and might easily forget all that was planned at discharge. Another participant emphasized that a caregiver who stayed with the patient at home was most preferred to those who just cared for them in the hospital and went away after discharge.
…we prefer the presence of a caretaker who is able to understand the information because sometimes you tell the old patient and he/she says, me I don’t still remember what you said. So it’s preferably better when the caregiver is around. That’s why you can now believe that you have passed on the right information to the right person. Some patients especially the elderly we know they have so many other cognitive diseases like dementia or any other that can affect their cognition and understanding. So in such cases we really need another person (caregiver) for a proper discharge plan. (Doctor, 47 years female)
Domain 3: Motivation
Barriers
Automatic Motivation: Poor Remuneration
Some participants expressed their concern about remuneration noting that if the remuneration of health workers was not good, they were not motivated to deliver the best quality of services. This indicated that for them to be motivated to do proper discharge planning, they needed to be remunerated well.
When you come to economic issues, you find that if you’re not remunerated nicely, mind wise you will not concentrate. Yes… so once the remuneration is nice, we also come happy and work happily and this patient will benefit and get a hundred percent of what he will need to have. So we really need some motivation part of it. (Nurse, 28 years male)
Reflective Motivation
Lack of Patient Follow-Up
Similarly, another participant reported that, however, much of the discharge planning may be good, lack of proper patient follow-up made health workers’ efforts worthless. The participant further explained that after properly discharging the patient, there were no arrangements to follow up the patient in the community thus uncertain whether there was continuity of care. As a result, patients are re-admitted when they were even worse than before.
There is a patient I discharged and she went home. Two years later, she was re-admitted having had a second amputation and she was in terrible pain. In such a case…I can’t say it was the discharge planning that caused the problems but I would say probably if there has been proper follow up and maybe continuous monitoring of the patient maybe every three months or so. Probably the patient would not have come in the state she came back in. (Physiotherapist, 30 years female)
Facilitators
Automatic Motivation: Desire for Patients’ Wellbeing
Some participants mentioned that they were moved to do proper discharge planning because of a strong desire for the patients’ wellbeing. One participant added that he tried to give science-based information to patients which could help them improve their wellbeing.
I mean the motivation to do all that is always there for every doctor because you want the patient to get well… (Doctor, 45 years male)
Am so confident to certain level with what I communicate to the patient because I communicate what the science tells me in regard to the care of the patient. Meaning that whatever I am communicating should improve the patient wellbeing. (Doctor, 34 years male)
Working Experience and Knowledge
Some participants mentioned that because they had handled patients with non-communicable diseases for a long time and had accumulated a lot of information regarding their care, they felt motivated to do proper discharge planning for the patients.
I think for the period I have been working with this department, I feel I have it all necessary to properly discharge those patients. I don’t know whether others can analyze and assess me differently but I feel I have the information that I can give them to support them maintain optimal health. (Nurse, 47 years female)
Reflective Motivation
Desire to Reduce Re-Admission of Recently Discharged Patients
Some participants stated that they were committed to carrying out proper discharge planning to reduce re-admission of the same patients. One participant noted that patients were commonly re-admitted due to failure to comply with or inadequate discharge planning. He added that on re-admission, patients were always worse than before. This therefore compelled some health workers to do a proper discharge plan the next time.
…if the discharge plan is inadequate, these patients are always re-admitted within even less than ten days. Because maybe one problem; drugs were missed or maybe the caregivers were not explained how to give a certain drug then they end up giving it wrongly and they (patients) end up coming back when they are sick and difficult to reverse. So, it’s really very important to do discharge planning. (Doctor, 31 years, male)
Discussion
This study found that at MRRH one of the Ugandan hospitals, discharge planning for older adults is mainly based on a hospital-specific discharge form or doctor opinion, as opposed to universal guidelines. The study found out that understaffing/workload/insufficient time was a significant setback of discharge planning. Nursing staff barely participate in the discharge process because they were few and engaged in other patient care roles. As a result of this, the few health workers available had little time for inter-professional consultation to develop a comprehensive discharge plan for the patient. Time was also insufficient for health workers to engage the patient and caregivers to give them detailed information about the discharge plan. In agreement to our study, Mizuma et al, Lapum et al20,21 and Coffey et al22 found out that lack of sufficient time and heavy workload hindered proper patient discharge.
Our study found that there was lack of interdisciplinary approach to discharge planning for instance; doctors and nurses worked in isolation during discharge of patients. According to evidence from previous studies, interdisciplinary discharge planning facilitates inter-professional communication and patient care after discharge.23 In addition, discharge planning should include interdisciplinary care coordination, a framework to guide communication, decision-making and continuous evaluation of discharge needs throughout patients’ hospital stay.24 Moreso, literature reveals that increasing nursing staff involvement in discharge process, clarifying interdisciplinary roles, putting guidelines for discharge planning and proper documentation of discharge care plan facilitate proper discharge planning.24 In such cases, a discharge coordinator was necessary to bridge the inter-professional communication gap. Previous studies have showed that presence of a discharge coordinator results in effective discharge planning through coordination of the multidisciplinary team. Authors further argued that a discharge coordinator reduces the work burden from the overwhelmed doctors and nurses.25,26 Previous studies have associated good interdisciplinary team work with effective discharge planning (Gholizadeh, Janati, Delgoshaei, Gorji, and Tourani, 2018 and Mennuni et al).27 Similarly, another study revealed that interdisciplinary approach improved the quality of care during transition from hospital-based to home-based care.28 However, health workers in this study reported a lack of a multidisciplinary approach to discharge planning. We found out that the decision to discharge a patient was made by a senior doctor (physician) only. Consistently,29 participants reported that only a physician could determine which patient to discharge without considering input of the rest of the healthcare team. Moreso, our institution does not involve a Comprehensive Geriatric Assessment (CGA), which is the major gap. All professionals are not directly involved in the care of older persons. As a result, the patients miss out on other professionals’ input which could improve discharge planning processes.
The study revealed a lack of written discharge policy or guidelines as a barrier to discharge planning. Under ideal circumstances, hospital leadership would play an essential role in designing and overseeing the implementation of a discharge planning policy and/or guidelines.30 The implementation of a streamlined discharge planning process is complex and requires significant commitment and focus from the hospital leadership and healthcare providers.31 Previous studies have reported that a well-implemented discharge policy has the potential to improve the hospital discharge process.32 However, our study found that no policy or guideline has been put in place at MRRH to be followed by healthcare providers during discharge and this calls for the hospital leadership’s prompt action to institute such discharge planning policies.
Similarly, there was inadequate documentation of the discharge plan instructions. Planning for discharge ought to begin at admission and patients need discharge notes with instruction guidelines well written to use after reaching home. Previous studies have strongly recommended that health workers need standardized guidelines for patient discharge and educational material for the caregivers.27 Related to our findings, studies have showed poor documentation during the discharge process.33 Consequently, essential steps or information might be omitted leading to ineffective discharge planning.34 However, our study revealed that a written piece of information not detailed with discharge instructions was given to patients or caregivers during discharge. As a result, patients forget the verbal instructions after reaching home. Since they lack written notes for reference, they end up not following the discharge plan. Related literature emphasizes that like other medical records, discharge plan should be documented and a copy provided to the patient.35
Family members demanded for discharge in some cases whether the patient was ready for discharge or not. Unplanned discharges are an important risk factor for poor outcomes. Such cases need better attention after discharge. Many families suffer catastrophic expenses during admission, some even selling property and often feel they have no choice but to leave. Thus, it is more of them leaving in the absence of medical advice. Our findings are related to findings from a study by Yong TY et al, 2013 who emphasized the need to pay greater attention to patients who went home against medical advice concerning their care before leaving the hospital since post-discharge outcomes to such patients are very poor.36 This is actually why early planning and engagement with family are important to better anticipate such challenges and prepare families for the transition from hospital- to community-based care early.
However, facilitators to discharge planning included but not limited to: Presence of patient caregiver was found to be a facilitating factor during discharge planning. This has been attributed to the essential roles played by the caregiver which include direct patient care, making patient care decision and acting on the behalf of the patient.25 In our study, we found that health workers preferred the caregiver to patient as a recipient of discharge instructions. They argued that patients’ memory retention is compromised by age and disease thus can easily forget the discharge instructions given to them. As a result, the presence of a regular caregiver would streamline the discharge planning process and if a caregiver is present, this can facilitate the transition to care at home easier.
In our study, healthcare providers reported that their long working experience in discharging older patients with non-communicable diseases enabled them to do it better. In line with our findings, a review of literature by Mizuma et al20 showed that health workers’ years of working experience in discharging older patients were associated with effective discharge planning. Similarly, another study among nurses reported a significant relationship between nurses’ experience and their participation in the discharge process.37 Due to extensive working experience, health workers continuously acquire knowledge and skills in proper discharge planning.
We found out that discharge planning was easier for patients with a regular caregiver or family support. This was because healthcare providers confidently relied on the caregivers to receive and implement discharge instructions on behalf of patients especially those with cognitive impairments like memory loss. Our findings are supported by previous study which emphasized that caregivers and family significantly contribute to proper discharge and continuity of care for older patients. The author added that the caregivers also participate in patient care decision-making process.25 In our study, caregivers guide the discharge medication prescription by considering their financial capacity to buy the medications.
Generally, this study indicated that barriers of discharge planning are far more than facilitators. This highlights the need for a multi-level reform and improvement of the discharge planning process to ensure adequate and sustainable patient care during and after hospitalization for better post-discharge outcomes of older adults.
Strengths and Limitations
This study employed the COM-B model to guide the data collection and analysis processes. This substantially enabled authors to identify barriers and facilitators of discharge planning from the health provider’s perspectives across all constituent domains (capability, opportunity and motivation) of the COM-B model. However, this study included healthcare providers’ perspective and did not include the perspective of patients and caregivers. It is the next step to further explore the patient and caregiver’s perspective concerning discharge planning. Also, this study was conducted in a single facility in Uganda, and the findings may not be generalized to other facilities in Uganda or in sub-Saharan Africa.
Conclusion
Discharge planning should not be seen as an event that begins and ends with the discharge summary, but instead as a process, which starts with the patient admission and develops throughout the hospitalization process. An effective management of hospital discharge requires the presence of health system/ level processes (like equipment, training, protocols, procedures), aimed at a systemic approach (organization), all together leading to positive outcomes for patient safety and satisfaction.
Abbreviations
MRRH, Mbarara Regional Referral Hospital; MUST, Mbarara University of Science and Technology; COM-B, Capacity; Opportunity Motivation Behavioural; LMIC, Low middle income country; SSA, Sub Saharan Africa.
Ethics Statement
This study was reviewed and approved by Mbarara University of Science and Technology Research Ethics Committee (MUST-2022-357) and the Uganda National Council of Science and Technology (HS2304ES). Administrative clearance was obtained from MRRH. The participants provided informed consent to participate in this study.
Acknowledgment
We thank the research assistants, Mbarara Regional Referral Hospital for all the support rendered to us towards the success of this study. We also appreciate the participants for accepting to participate in this study.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, analysis and interpretation of data; took part in drafting the article, revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Funding
Research reported in this publication was supported by the Fogarty International Center of National Institutes of Health under Award Number D43TWO11632. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Disclosure
Ms Judith Owokuhaisa reports grants from Mbarara University of Science and Technology Uganda, during the conduct of the study. The authors declare that they have no other conflicts of interest in this work.
References
1. Karlsson SG, Jönsson JH. Forced migration, older refugees and displacement: implications for social work as a human rights profession. J Hum Rights Soc Work. 2020;5(3):212–222. doi:10.1007/s41134-020-00120-6
2. Mayega RW, Guwatudde D, Makumbi F, et al. Diabetes and pre-diabetes among persons aged 35 to 60 years in eastern Uganda: prevalence and associated factors. PLoS One. 2013;8(8):e72554. doi:10.1371/journal.pone.0072554
3. Prince MJ, Wu F, Guo Y, et al. The burden of disease in older people and implications for health policy and practice. Lancet. 2015;385(9967):549–562. doi:10.1016/S0140-6736(14)61347-7
4. Orikiriza P, Rukundo GZ, Kayanja A, Bazira J. clinical conditions of hospitalized older adult patients and their outcomes in a regional referral hospital in Southwestern Uganda. J Aging Res. 2020;2020:1–6. doi:10.1155/2020/6830495
5. Madigan EA, Gordon NH, Fortinsky RH, Koroukian SM, Piña I, Riggs JS. Rehospitalization in a national population of home health care patients with heart failure. Health Serv Res. 2012;47(6):2316–2338. doi:10.1111/j.1475-6773.2012.01416.x
6. Lin C-J, Cheng S-J, Shih S-C, Chu C-H, Tjung -J-J. Discharge planning. Int J Gerontol. 2012;6(4):237–240. doi:10.1016/j.ijge.2012.05.001
7. Shepperd S, Lannin NA, Clemson LM, McCluskey A, Cameron ID, Barras SL. Discharge planning from hospital to home. Cochrane Database Syst Rev. 2013;2013:1.
8. Mckeehan KM, Coulton C. A systems approach to program development for continuity of care in hospitals. Contin Care. 1985;10:1.
9. Wertheimer DS, Kleinman LS, Kleinman LS. A model for interdisciplinary discharge planning in a university hospital. Gerontologist. 1990;30(6):837–840. doi:10.1093/geront/30.6.837
10. Needham DM, Davidson J, Cohen H, et al. Improving long-term outcomes after discharge from intensive care unit: report from a stakeholders’ conference. Crit Care Med. 2012;40(2):502–509. doi:10.1097/CCM.0b013e318232da75
11. Wiens M, Kumbakumba E, Larson C, et al. Postdischarge mortality in children with acute infectious diseases: derivation of postdischarge mortality prediction models. BMJ open. 2015;5(11):e009449. doi:10.1136/bmjopen-2015-009449
12. McDonagh LK, Saunders JM, Cassell J, et al. Application of the COM-B model to barriers and facilitators to chlamydia testing in general practice for young people and primary care practitioners: a systematic review. Implemen Sci. 2018;13(1):1–19. doi:10.1186/s13012-018-0821-y
13. Wiltsey Stirman S, Baumann AA, Miller CJ. The FRAME: an expanded framework for reporting adaptations and modifications to evidence-based interventions. Implemen Sci. 2019;14(1):1–10. doi:10.1186/s13012-019-0898-y
14. Orb A, Eisenhauer L, Wynaden D. Ethics in qualitative research. J Nurs Scholarsh. 2001;33(1):93–96. doi:10.1111/j.1547-5069.2001.00093.x
15. Sutton J, Austin Z. Qualitative research: data collection, analysis, and management. Can J Hosp Pharm. 2015;68(3):226. doi:10.4212/cjhp.v68i3.1456
16. Ruona WE. Analyzing qualitative data. Res Organ. 2005;223(263):233–263.
17. Groenland E. Employing the matrix method as a tool for the analysis of qualitative research data in the business domain. Int J Bus Glob. 2018;21(1):119–134. doi:10.1504/IJBG.2018.094106
18. Fereday J, Muir-Cochrane E. Demonstrating rigor using thematic analysis: a hybrid approach of inductive and deductive coding and theme development. Int J Qual Methods. 2006;5(1):80–92. doi:10.1177/160940690600500107
19. Hsieh H-F, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–1288. doi:10.1177/1049732305276687
20. Mizuma K, Amitani M, Mizuma M, et al. Clarifying differences in viewpoints between multiple healthcare professionals during discharge planning assessments when discharging patients from a long-term care hospital to home. Eval Program Plann. 2020;82:101848. doi:10.1016/j.evalprogplan.2020.101848
21. Lapum JL, Fredericks S, Liu L, et al. Facilitators and barriers of heart surgery discharge: patients’ and nurses’ narrative accounts. J Cardiovas Nurs. 2016;31(4):350–356. doi:10.1097/JCN.0000000000000253
22. Coffey A, Leahy-Warren P, Savage E, et al. Interventions to promote early discharge and avoid inappropriate hospital (re) admission: a systematic review. Int J Environ Res Public Health. 2019;16(14):2457. doi:10.3390/ijerph16142457
23. Okoniewska B, Santana MJ, Groshaus H, et al. Barriers to discharge in an acute care medical teaching unit: a qualitative analysis of health providers’ perceptions. J Multidiscip Healthc. 2015;8:83. doi:10.2147/JMDH.S72633
24. McNeil A. Using evidence to structure discharge planning. Nurs Manage. 2016;47(5):22–23. doi:10.1097/01.NUMA.0000482502.28559.b1
25. Bauer M, Fitzgerald L, Haesler E, Manfrin M. Hospital discharge planning for frail older people and their family. Are we delivering best practice? A review of the evidence. J Clin Nurs. 2009;18(18):2539–2546. doi:10.1111/j.1365-2702.2008.02685.x
26. Ou L, Chen J, Young L, Santiano N, Baramy L-S, Hillman K. Effective discharge planning–timely assignment of an estimated date of discharge. Aust Health Rev. 2011;35(3):357–363. doi:10.1071/AH09843
27. Mennuni M, Gulizia MM, Alunni G, et al. ANMCO position paper: hospital discharge planning: recommendations and standards. Eur Heart J Suppl. 2017;19(suppl_D):D244–D55. doi:10.1093/eurheartj/sux011
28. Wang Y-C, Lee W-Y, Chou M-Y, et al. Cost and effectiveness of long-term care following integrated discharge planning: a prospective cohort study.
29. Simbolon S, Hamid AYS. The effectiveness of discharge planning stroke patient due to hypertension to improve patient satisfaction and Independence. Enfermeriaclinica. 2019;29:703–708.
30. Gholizadeh M, Janati A, Delgoshaei B, Gorji HA, Tourani S. Implementation requirements for patient discharge planning in health system: a qualitative study in Iran. Ethiop J Health Sci. 2018;28(2):157–168. doi:10.4314/ejhs.v28i2.7
31. Mitchell SE, Martin J, Holmes S, et al. How hospitals reengineer their discharge processes to reduce readmissions. J Healthcare Qual. 2016;38(2):116. doi:10.1097/JHQ.0000000000000005
32. Kabajaasi O, Trawin J, Derksen B, et al. Transitions from hospital to home: a mixed methods study to evaluate pediatric discharges in Uganda. PLOS Glob Public Health. 2023;3(9):e0002173. doi:10.1371/journal.pgph.0002173
33. Graham J, Gallagher R, Bothe J. Nurses’ discharge planning and risk assessment: behaviours, understanding and barriers. J Clin Nurs. 2013;22(15–16):2338–2346. doi:10.1111/jocn.12179
34. Horstman MJ, Mills WL, Herman LI, et al. Patient experience with discharge instructions in postdischarge recovery: a qualitative study. BMJ Open. 2017;7(2):e014842. doi:10.1136/bmjopen-2016-014842
35. Andrew NE, Busingye D, Lannin NA, Kilkenny MF, Cadilhac DA. The quality of discharge care planning in acute stroke care: influencing factors and association with postdischarge outcomes. J Stroke Cerebrovasc Dis. 2018;27(3):583–590. doi:10.1016/j.jstrokecerebrovasdis.2017.09.043
36. Yong T, Fok J, Hakendorf P, Ben‐Tovim D, Thompson C, Li J. Characteristics and outcomes of discharges against medical advice among hospitalised patients. Intern Med J. 2013;43(7):798–802. doi:10.1111/imj.12109
37. Facchinetti G, Ianni A, Piredda M, et al. Discharge of older patients with chronic diseases: what nurses do and what they record. An observational study. J Clin Nurs. 2019;28(9–10):1719–1727.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.