")
Back to Journals » International Journal of Women's Health » Volume 14
Pregnant and Breastfeeding Women’s Attitudes and Fears Regarding COVID-19 Vaccination: A Nationwide Cross-Sectional Study in Saudi Arabia
Authors Alshahrani SM , Alotaibi A, Almajed E , Alotaibi A, Alotaibi K, Albisher S
Received 29 August 2022
Accepted for publication 17 November 2022
Published 25 November 2022 Volume 2022:14 Pages 1629—1639
DOI https://doi.org/10.2147/IJWH.S387169
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Sultan M Alshahrani,1 Amjad Alotaibi,2 Ebtesam Almajed,2 Aisha Alotaibi,2 Kholoud Alotaibi,2 Sara Albisher3
1Department of Neurosciences, King Abdullah bin Abdulaziz University Hospital, Princess Nourah Bint Abdulrahman University, Riyadh, Saudi Arabia; 2College of Medicine, Princess Nourah Bint Abdulrahman University, Riyadh, Saudi Arabia; 3College of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia
Correspondence: Sultan M Alshahrani, Department of Neurosciences, King Abdullah bin Abdulaziz University Hospital, Princess Nourah Bint Abdulrahman University, Airport Road, Riyadh, 11564, Saudi Arabia, Tel +966-112803212, Fax +966-112800000, Email [email protected]
Introduction: Contracting coronavirus disease (COVID-19) during pregnancy has been linked to an increased risk of severe maternal and fetal complications. Mass vaccination is considered a promising solution to successfully combat the COVID-19 pandemic. It includes vaccinating of pregnant and breastfeeding women. The success of a vaccine is determined not only by its efficacy, but also by its acceptability. Therefore, our study aimed to explore the acceptability and reluctance of pregnant and breastfeeding women to receive COVID-19 vaccination in Saudi Arabia.
Methods: This cross-sectional study was conducted in Saudi Arabia from March 2022-beginning to June 2022-end. Using an online self-administered questionnaire with a convenience sampling technique, we assessed women for pregnancy, gravidity, parity, high-risk pregnancy, trimester of pregnancy, and current or planned breastfeeding. Furthermore, we assessed patients with preexisting chronic illnesses. The questionnaire comprised sociodemographic data and items drawn from Goncu Ayhan et al, including vaccination history, perception of risk related to the COVID-19 pandemic, impact of the COVID-19 pandemic, and acceptance and attitude toward future COVID-19 vaccination.
Results: A total of 854 women (615 pregnant and 192 breastfeeding women) were included. Predictors of COVID-19 vaccination acceptance were found in women with a high level of education, those who lived with an elderly family member, and had close contact with a COVID-19-positive person. The reasons for declining vaccination included COVID-19 diagnosis during pregnancy and concerns about side effects of COVID-19 vaccines. A total of 503 (58.9%) women believed that COVID-19 vaccines had the potential to harm their babies. Only 415 (48.6%) agreed they would take the COVID-19 vaccine if it were recommended for pregnant women.
Conclusion: Pregnant and breastfeeding women fear COVID-19 vaccination due to safety concerns for their babies. COVID-19 vaccine acceptance varies among pregnant and breastfeeding women, regardless of whether they receive the COVID-19 vaccine. Our study underlines the importance of public education campaigns to improve the overall quality of information on COVID-19 vaccination, particularly among pregnant and breastfeeding women.
Keywords: COVID-19, fears, vaccine, pregnant, breastfeeding, Saudi women
Introduction
According to the World Health Organization (WHO), as of August 11, 2022, there were over 585 million confirmed cases of COVID-19, including six million deaths worldwide.1 Contracting COVID-19 during pregnancy has been linked to an increased risk of severe maternal and fetal complications, such as maternal admissions to the Intensive Care Unit and risk of mechanical ventilation, comorbidities like preeclampsia and thrombosis, maternal mortality, preterm births, and stillbirths.2 Therefore, the prevention of coronavirus disease should be a top priority for pregnant and breastfeeding women. Preventative measures against COVID-19 include social distancing, mandatory facemasks, and regular hand hygiene.3 However, vaccination is considered a crucial factor in successfully combating the COVID-19 pandemic.4,5 Pregnant and breastfeeding women are considered to be high-risk populations. They need to be closely monitored for the prevention and management of COVID-19. Clinical practice guidelines for the prevention and management of COVID-19 (SARS-CoV-2) infection during pregnancy have been developed by many health organizations.6 These guidelines also recommend booster doses for the prevention of COVID-19 during pregnancy. The Saudi Ministry of Health has been following these guidelines’ recommendations, has provided COVID-19 vaccination for all populations, and has made high-risk populations a priority for vaccination.7
A prospective study conducted in Ankara City Hospital in Turkey at the beginning of 2021 revealed that among the 300 women participants, only 37% were willing to get the COVID-19 vaccine. Their low acceptance of the vaccine was attributed to insufficient data on COVID-19 vaccine safety for pregnant women and the potential harm to the fetus.8 According to this study, accepting the COVID-19 vaccination was found to have a slightly positive connection with the number of school-aged children. Additionally, pregnant women were more accepting of COVID-19 immunization in the first trimester than in the second and third trimesters. Another cross-sectional study investigated the attitudes and fears regarding COVID-19 vaccination among pregnant and breastfeeding women in Germany.2 According to the findings, most women (57.4%) out of 2339 participants were not in favor of receiving the COVID-19 vaccine. The acceptability of the COVID-19 vaccine was higher in the breastfeeding group. However, many women were either unsure of or opposed to receiving the vaccine. Additionally, this study clarified the reasons for vaccination hesitancy in both groups, including women’s perception of limited vaccination-specific information, limited scientific evidence on vaccination safety, and the fear of harming the fetus or infant that may lead to pregnancy complications. Additionally, the study showed that in both categories, women’s willingness to be vaccinated was linked to their fear of infection and the likelihood of developing disease symptoms, and greater vaccine acceptance was linked to increased concern about getting the infection and its severe symptoms.2 Another study conducted in the Mecca Province of Saudi Arabia9 evaluated the acceptance rate of the COVID-19 vaccine among pregnant women and those planning for pregnancy. The women obtained a moderate score regarding the COVID-19 vaccine’s perception, hesitancy, and its possible benefits. The study elaborated on the possible reasons behind participants’ unwillingness to get vaccinated against the coronavirus, including uncertainty regarding vaccine safety and effectiveness in pregnant women. Several professional organizations, including the American College of Obstetricians and Gynecologists (ACOG), Royal College of Obstetricians and Gynecologists (RCOG), Centers for Disease Control and Prevention (CDC), and Society for Maternal-Fetal Medicine (SMFM), have stressed the importance of COVID-19 vaccination during pregnancy and breastfeeding phase.10 Since the vaccine’s success is determined not only by its efficacy but also by its acceptability, this study aimed to explore the acceptability and reluctance of COVID-19 vaccination among pregnant and breastfeeding women in Saudi Arabia.
Methods
Study Population
A descriptive cross-sectional study was conducted to determine the acceptance and reluctance of COVID-19 vaccination in the Saudi Arabian population of pregnant and breastfeeding women through an anonymous online questionnaire using the convenience sampling technique. The study was conducted from the beginning of March 2022 to the end of June 2022. The inclusion criteria were: women living in Saudi Arabia, aged 18 years and above, and willing to participate. The sample size was estimated using G-power software with a confidence level of 95%, and an error margin of ±5%, and 25% of the total sample size was added to compensate for the non-response rate; the minimum sample size required was 800 participants. The total sample size was 854.
Ethics Statement & Informed Consent
Ethical approval for this study was obtained from the Institutional Review Board (IRB) of Princess Nourah bint Abdulrahman University (PNU), Riyadh, Saudi Arabia (IRB log number:22–0097). Informed consent was obtained from all participants before conducting the study. All participants were briefed on the research goals and were informed that they could withdraw from the study with no repercussions.
Study Survey
The study survey was created and the data collected using a Google Form, which was then distributed randomly across various social media platforms (WhatsApp, Telegram, and Twitter) as well as by the official e-mail service at PNU and King Abdullah bin Abdulaziz University Hospital (KAAUH).
First, a group of four native Arabic language experts independently translated the scale into Arabic. The draft translation of the questionnaire was then reviewed, checked for accuracy and cultural suitability, and approved by a mental health and non-mental health professional. Finally, the draft was back-translated into English by a qualified professional translator. The questionnaire consisted of the following sections: (a) sociodemographic data including age, gender, nationality, educational level, current residency, marital status, occupational status, average monthly income, gravidity, parity (primi/multi), gestational age, breastfeeding status, for the pregnancy group we inquired if they planned to breastfeed, presence of high-risk pregnancy, and preexisting chronic illness to help classify participants at high risk of acquiring severe COVID-19 infections. (b) A questionnaire from Ayhan et al was used.8 It consisted of 28 items in which participants were questioned about vaccination history (including COVID-19, influenza, and tetanus vaccines), perception of risk related to the COVID-19 pandemic, the impact of the COVID-19 pandemic, self-discipline on preventive measures against COVID-19, acceptance, and attitude toward future COVID-19 vaccination.
We assessed sociodemographic variables including age, area of residence, education, occupation, and average monthly income. We also assessed current health status looking for chronic illnesses and diagnosed COVID-19 infection in the past. Subsequently, we asked about pregnancy and breastfeeding. Other questions include gestational age, high-risk pregnancy, number of pregnancies and previous pregnancies’ outcome, and the plan to breastfeed if currently pregnant. We also asked about the age of the child in the breastfeeding women. We then posed the same questions to both groups regarding vaccinations against COVID-19 and influenza. Additionally, we assessed the anxiety associated with COVID-19 and its symptoms. Moreover, we assessed the discipline of precautionary measures against COVID-19 and general knowledge of the virus. Finally, we assessed the participants’ attitudes and practices related to COVID-19 vaccination. The main outcome of this study is the acceptance and reluctance among pregnant and breastfeeding women to COVID-19 vaccination in Saudi Arabia. We also explored the same outcome in women with high-risk pregnancies, defined as any pregnancy that involves increased health risks for the pregnant person, fetus, or both.
Statistical Analysis and Data Management
All collected data were tabulated on a Microsoft Excel sheet and then transferred to IBM Statistical Package for Social Sciences, Version 23 (SPSS Inc., Chicago, IL, USA) for data analysis. Descriptive statistics in the form of frequencies and percentages, using suitable tables and figures, were used to represent categorical data. Pearson’s chi-square test was used to test the association between categorical variables. Statistical significance was set at P < 0.05.
Results
We received responses from 854 women residing in various provinces of Saudi Arabia [Table 1]. The study population comprised 615 (72%) pregnant and 192 (22.5%) breastfeeding women. Sociodemographic analysis showed that 463 (54.2%) were 26–35 years, 824 (96.5%) married, 505 (59.1%) unemployed, and 773 (93.8%) were supported by their husbands. 132 (15.5%) had chronic illnesses. The most reported chronic illnesses were thyroid disease (6%), hypertension (2.8%), and diabetes (2.8%). Among the pregnant women, 112 (13.1%) had a high-risk pregnancy. Among those who were currently pregnant, 95.9% reported planning to breastfeed their babies after delivery. Of the 27 (4.1%) women who were not planning to breastfeed, the most commonly cited reasons were work (11.1%), health issues (11.1%), and tiredness (11.1%). A total of 192 (22.5%) women reported that they currently breastfeed and the most common reason for not breastfeeding was “currently pregnant”, whereas 86.4% did not have any particular reason not to breastfeed. The sociodemographic data, pregnancy status, and breastfeeding characteristics are presented in [Table 1].
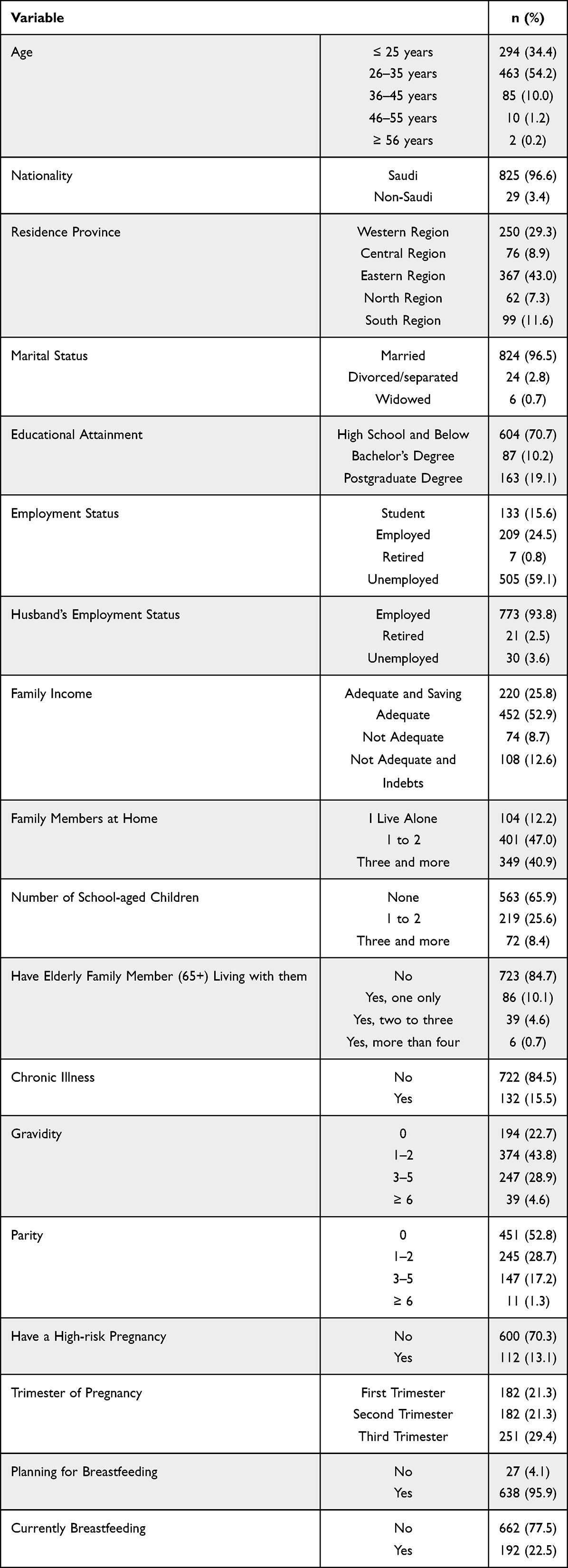 |
Table 1 Sociodemographic, Pregnancy and Breastfeeding Related Characteristics of Study Sample, n = 854 |
The attitudes, perceptions, and practices related to vaccination of the participants are presented in [Table 2]. In the past five years, 636 (74.5%) women had received other vaccine brands. A total of 732 (85.7%) women believed that they had sufficient information about the COVID-19 vaccine, but 400 (46.8%) reported that they lacked knowledge about COVID-19 vaccine safety during pregnancy and/or breastfeeding. Moreover, 503 (58.9%) women thought that the COVID-19 vaccine carries the possibility of harm to their babies. However, 415 (48.6%) women reported that if the COVID-19 vaccine was recommended for pregnant and breastfeeding women, they would receive it. Overall, 795 (93.1) women received at least two doses of the COVID-19 vaccine based on governmental requirements.
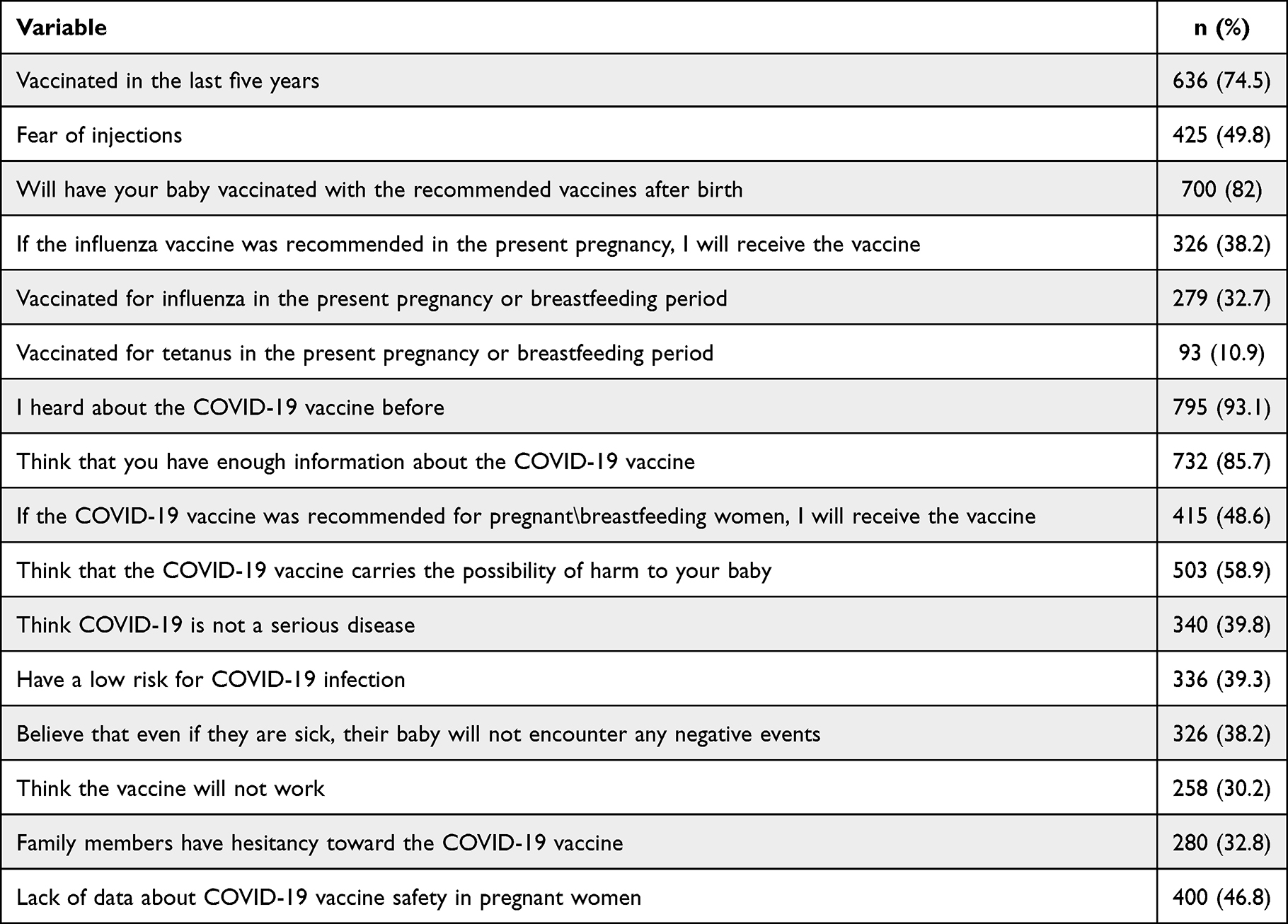 |
Table 2 Participants’ Attitudes, Perceptions and Practices Related to Vaccination |
COVID-19 vaccine acceptance was in 301 (72.5%) pregnant women, 50 (12%) women with high-risk pregnancies, and 64 (15.4%) breastfeeding women. In contrast, COVID-19 vaccine non-acceptance in the same group was in 299 (68.1), 62 (14.1), and 78 (17.8) women, respectively [Table 3]. When we evaluated the relationship between COVID-19 precautions with pregnancy risk and breastfeeding women, close contact with a COVID-19-positive person was statistically significant (p=0.014), indicating that it was a predictor of COVID-vaccine acceptance. Additionally, no statistically significant association was observed between COVID-19 acceptance and high-risk pregnancies (p=0.368) [Table 3].
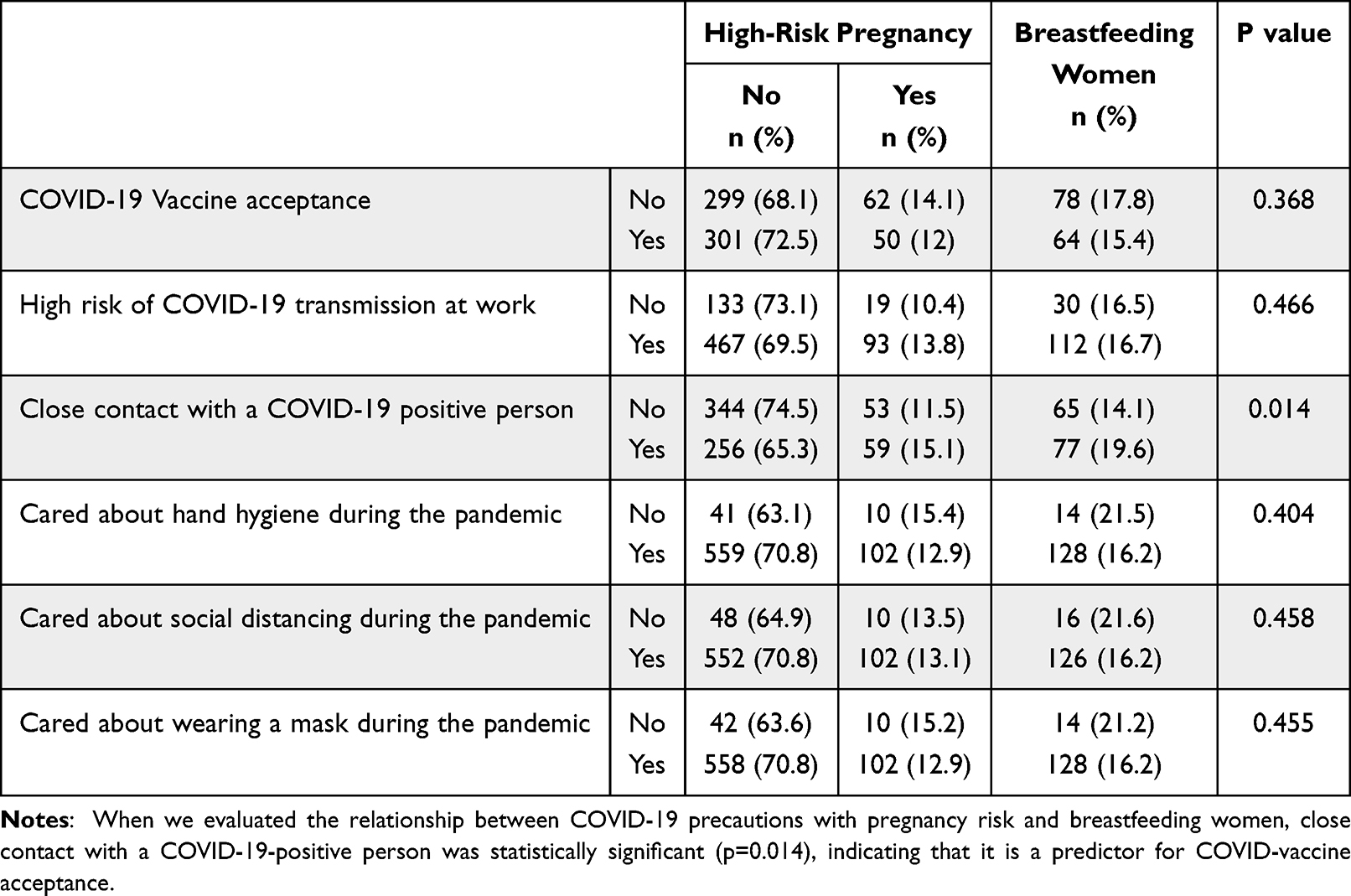 |
Table 3 COVID-19 Precautions of Pregnant and Breastfeeding Women |
The relationships between COVID-19 vaccine acceptance and sociodemographic, pregnancy, breastfeeding, and family-related characteristics are shown in [Table 4]. Women with a high level of education had statistically significant acceptance (p=0.011) of the COVID-19 vaccine compared to women with a lower level of education. Moreover, women who had elderly family members (aged above 65 years) living with them had statistically significant (p=0.030) acceptance of the COVID-19 vaccine compared to women who did not have elderly family members at home. No statistically significant relationships were observed between COVID-19 vaccine acceptance and age (p=0.709), nationality (p=0.429), current residency (p=0.370), marital status (p=0.624), occupation status (p-0.462), husband’s occupation status (p=0.077), and family income (p=0.150). Moreover, there was no statistically significant association observed with the trimester of pregnancy (p=0.078), currently breastfeeding (p=0.826), number of family members at home (p=0.534), and number of school-age children (p=0.534).
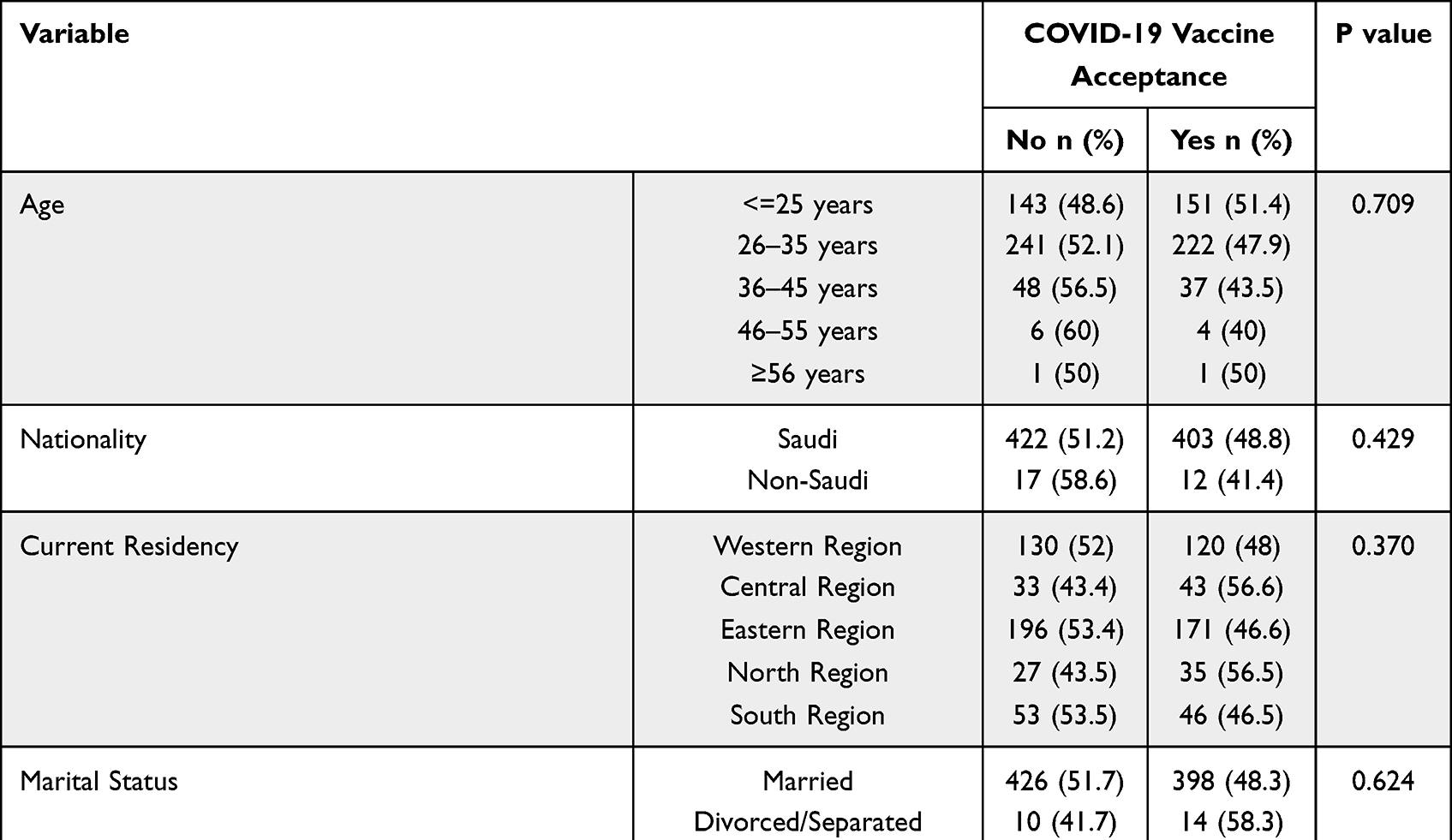 |
Table 4 Relationship Between COVID-19 Vaccine Acceptance and Sociodemographic, Pregnancy, Breastfeeding and Family Characteristics |
Discussion
Our study assessed 854 women: 615 (72%) pregnant and 192 (22.5%) breastfeeding. The study found that pregnant and breastfeeding women feared COVID-19 vaccination due to uncertainty over its safety for their babies during pregnancy and breastfeeding. Moreover, due to international and governmental regulations by the Ministry of Health in Saudi Arabia, COVID-19 vaccine acceptance was variable among pregnant and breastfeeding women. We assessed COVID-19 vaccine acceptance versus non-acceptance in this group. It showed variable positive and negative responses based on their knowledge of COVID-19 and the effectiveness and safety of the COVID-19 vaccine. However, most women received at least two doses of the COVID-19 vaccine following governmental requirements. We also found that predictors of COVID-19 vaccination acceptance were women with a high level of education, having an elderly family member living with them at home, and having close contact with a COVID-19-positive person.
Such findings may contradict their perceptions and fears regarding the vaccine. This can be explained by the fact that women fear the COVID-19 vaccine; however, they are obliged to take it.7 Moreover, the Saudi Health Authority obliges citizens to be vaccinated to go to workplaces, schools, universities, and other social activities.
To the best of our knowledge, this is the largest study on pregnant and breastfeeding women’s perspectives regarding the COVID-19 vaccine. Our findings appear to reflect Saudi women’s perspectives based on the size of the studied sample and the demographics that we observed. Nevertheless, we recognize as a limitation that the results of this study may not be appropriate to extrapolate to other countries because of the differences in the handling and distribution of the COVID-19 vaccine, for each country is developing its own strategic vaccination plan. However, we suggest that the findings regarding the influence of anxiety levels on vaccination willingness and the need for credible studies demonstrating the safety of vaccination in pregnant and breastfeeding women be generalized.
The low acceptance rate of COVID-19 vaccine during pregnancy and breastfeeding underlines the importance of scientific studies to investigate the safety of COVID-19 vaccination for pregnant and breastfeeding women to increase trust in and acceptance of vaccinations. Furthermore, the present findings confirm the necessity of public education campaigns to improve the overall quality of information on COVID-19 vaccination, particularly among pregnant and breastfeeding women.
Our study is consistent with what has been reported in previous studies in Germany, Turkey, and Italy.2,8,11 Among the participants of this study, a high percentage of pregnant women believed that they were at considerable risk of SARS-CoV-2. The Centers for Disease Control and Prevention (CDC) listed pregnancy as a risk factor for severe COVID-19, even though the absolute risk of SARS-CoV-2 severe infection is low.12 Currently, there are no approved vaccines for pregnant or breastfeeding women, because these groups are excluded from clinical trials and there is a scarcity of information about the efficacy of COVID-19 vaccines on pregnant women. The vaccination of pregnant women against SARS-CoV-2 remains controversial owing to the lack of data on the vaccine’s safety and efficacy for the developing fetus as well as the newborn baby.
A systematic review and meta-analysis of 11 studies published in 2022 that explored the uptake of COVID-19 vaccinations among pregnant women found that the factors that predicted COVID-19 vaccination uptake in pregnant women were older age, ethnicity, race, fear of COVID-19 during pregnancy, and trust in COVID-19 vaccines. Additionally, they illustrated the common reasons for declining vaccination, which include diagnosis of COVID-19 during pregnancy, mistrust in the government, and concerns about the safety and side effects of COVID-19 vaccines for both mothers and newborns. The studies corroborate our results, except for mistrust in the government, which was not a reason for declining vaccination in the studied sample.13 Our findings showed that younger pregnancy/breastfeeding women had a higher acceptance of COVID-19 vaccines, which is in contrast with the findings of several studies where they stated that older age is related to higher acceptance of COVID-19 vaccines.14–16 Moreover, participants’ fear of infection and the likelihood of developing severe disease symptoms were linked to their acceptance of the vaccine. A positive association was found between acceptance of the COVID-19 vaccine and the number of elderly family members in the household (P=0.03). Participants in households with elderly family members expressed higher anxiety about the risk of transmission by household members to the elderly, who are by far the most vulnerable population group.17 COVID-19 has a higher mortality rate in elderly patients than in young and middle-aged patients.18 In the studied sample, participants who had elderly family members accepted the COVID-19 vaccine compared to those with no elderly family members. In Germany, a cross-sectional study carried out at the beginning of 2021 revealed that vaccine acceptance was higher among breastfeeding women than among pregnant women.2 This finding was inconsistent with our findings. We did not find difference in COVID-19 vaccine acceptance between breastfeeding and pregnant women. In terms of the relationship between COVID-19 vaccine acceptance and sociodemographic characteristics, the education level in Czech pregnant women significantly predicted their vaccination uptake and their attitude toward professional recommendations, a finding that is consistent with our results.19
It is important to consider the perspective of pregnant and breastfeeding women when making decisions on vaccination recommendations and information policies for COVID-19 vaccines. Pregnant women are understandably nervous about getting the vaccine because they are worried that it would harm their unborn children or cause birth defects. The majority of women who were not in favor of receiving the COVID-19 vaccine in the present study were due to their lack of knowledge about the safety and efficacy of the COVID-19 vaccine.
As reported by the CDC, the decision to receive vaccination during gestation and breastfeeding should be made on an individual basis, taking into account both the advantages and possible risks. Hence, obstetricians must update their knowledge regarding the recent developments in the safety of the COVID-19 vaccine and the complications that COVID-19 poses to pregnant women. Obstetricians should address the benefits and potential risks of the vaccine with women who have risk factors (ie, advanced age (>35 years), a higher BMI, and hypertension) to allow a collaborative choice according to their individual conditions.20,21 Pregnant women’s anxiety and stress levels rose during the pandemic, demonstrating the pandemic’s psychological impact on this vulnerable subgroup.22–24 Thereby, obstetricians must take patients’ worries seriously and do their best to educate and counsel them suitably.
As demonstrated by our statistics, only 48.6% of women agreed for vaccination against SARS-CoV-2 if it was recommended during pregnancy, while 57% of women were concerned about the possible health consequences for their baby and 30.2% were concerned about the vaccine’s efficacy. The extent to which vaccines could reliably prevent the potential problems of COVID-19 infection during pregnancy, such as increased maternal morbidity, mortality, and premature birth.25,26 Although studies illustrate that the vaccine is safe, it is expected that pregnant and breastfeeding women will benefit from the vaccine to safeguard their unborn and infant children and achieve herd immunity to help halt the pandemic.27 However, it is important to conduct a follow-up study to see how pregnant and breastfeeding women respond to the vaccine once studies have been published on its safety.
Pregnant and breastfeeding women are considered to be high-risk populations. Counselling and educating them about COVID-19 vaccination is imperative to preventing unwanted pregnancy and birth outcomes. A recent systematic review and meta-analysis of clinical practice guidelines for the prevention and management of COVID-19 (SARS-CoV-2) infection during pregnancy have been developed by many health organizations.6
Limitations
The present study has some limitations. These include (i) the use of non-probability sampling, which may limit the generalizability of our results; (ii) the cross-sectional design of the study; the results reflect associations rather than causation; and (iii) the online distribution of the questionnaire, which may affect the representativeness of the study sample. Nonetheless, based on recent data from the World Bank Database, approximately 98% of the Saudi population uses the Internet, which implies it is widely available and readily accessible.28 Additionally, the questionnaire used self-created items to assess attitudes and perceptions regarding COVID-19 vaccination and anxiety levels related to the attitude and acceptance of vaccination rather than validated questionnaires. However, currently, there is no validated questionnaire to assess COVID-19 infection anxiety levels.
Conclusion
Our study highlights the importance of implementing public education campaigns to improve the overall quality of information on COVID-19 vaccination, particularly among pregnant and breastfeeding women. Counseling and educating pregnant and breastfeeding women about COVID-19 vaccination is essential to prevent unwanted pregnancy and birth outcomes.
Data Sharing Statement
Data from this study is available for sharing on request.
Acknowledgments
The authors would like to acknowledge and express their sincere gratitude to the volunteers who helped with data collection, the participants for their cooperation, and the Research and Academic Accreditation Office of Princess Nourah bint Abdulrahman University (PNU) and King Abdullah bin Abdulaziz University Hospital (KAAUH) for their help in distributing the survey to all staff members. This study could not have been completed without data collection efforts.
Funding
The authors received no financial support for this research, authorship, or publication of this article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. WHO COVID-19 Dashboard. Geneva: World Health Organization; 2020. Available from: covid19.who.int/.
2. Schaal NK, Zöllkau J, Hepp P, Fehm T, Hagenbeck C. Pregnant and breastfeeding women’s attitudes and fears regarding the COVID-19 vaccination. Arch Gynecol Obstet. 2022;306(2):365–372. doi:10.1007/s00404-021-06297-z
3. Munnoli PM, Nabapure S, Yeshavanth G. Post-COVID-19 precautions based on lessons learned from past pandemics: a review. J Public Health. 2022;30:973–981. doi:10.1007/s10389-020-01371-3
4. Ciotti M, Ciccozzi M, Terrinoni A, Jiang WC, Wang CB, Bernardini S. The COVID-19 pandemic. Crit Rev Clin Lab Sci. 2020;57(6):365–388. doi:10.1080/10408363.2020.1783198
5. Sharma O, Sultan AA, Ding H, Triggle CR. A review of the progress and challenges of developing a vaccine for COVID-19. Front Immunol. 2020;11:585354. doi:10.3389/fimmu.2020.585354
6. Di Girolamo R, Khalil A, Rizzo G, et al. Systematic review and critical evaluation of quality of clinical practice guidelines on the management of SARS-CoV-2 infection in pregnancy. Am J Obstet Gynecol. 2022;4:100654.
7. Ministry of Health. Kingdom of Saudi Arabia © 2022: COVID-19 Vaccine. Available from: https://www.moh.gov.sa/en/awarenessplateform/VariousTopics/Pages/COVID-19Vaccine.aspx.
8. Goncu Ayhan S, Oluklu D, Atalay A, et al. COVID-19 vaccine acceptance in pregnant women. Int J Gynecol Obstet. 2021;154:291–296. doi:10.1002/ijgo.13713
9. Samannodi M. COVID-19 vaccine acceptability among women who are pregnant or planning for pregnancy in Saudi Arabia: a cross-sectional study. Patient Prefer Adherence. 2021;15:2609–2618. doi:10.2147/PPA.S338932
10. Kuciel N, Mazurek J, Hap K, Marciniak D, Biernat K, Sutkowska E. COVID-19 vaccine acceptance in pregnant and lactating women and mothers of young children in Poland. Int J Womens Health. 2022;14:415–424. doi:10.2147/IJWH.S348652
11. Carbone L, Mappa I, Sirico A, et al. Pregnant women’s perspectives on severe acute respiratory syndrome coronavirus 2 vaccine. Am J Obstet Gynecol MFM. 2021;3(4):100352. doi:10.1016/j.ajogmf.2021.100352
12. Zambrano LD, Ellington S, Strid P. Update: characteristics of symptomatic women of reproductive age with laboratory-confirmed SARS-CoV-2 infection by pregnancy status - United States, January 22-October 3, 2020. MMWR Morb Mortal Wkly Rep. 2020;69:1641–1647. doi:10.15585/mmwr.mm6944e3
13. Galanis P, Vraka I, Siskou O, Konstantakopoulou O, Katsiroumpa A, Kaitelidou D. Uptake of COVID-19 vaccines among pregnant women: a systematic review and meta-analysis. Vaccines. 2022;10(5):766. doi:10.3390/vaccines10050766
14. Skjefte M, Ngirbabul M, Akeju O, et al. COVID-19 vaccine acceptance among pregnant women and mothers of young children: results of a survey in 16 countries. Eur J Epidemiol. 2021;36:197–211. doi:10.1007/s10654-021-00728-6
15. Levy AT, Singh S, Riley LE, Prabhu M. Acceptance of COVID-19 vaccination in pregnancy: a survey study. Am J Obstet Gynecol. 2021;3:100399.
16. Stuckelberger S, Favre G, Ceulemans M, et al. SARS-CoV-2 vaccine willingness among pregnant and breastfeeding women during the first pandemic wave: a cross-sectional study in Switzerland. Viruses. 2021;13:1199. doi:10.3390/v13071199
17. Daoust JF. Elderly people and responses to COVID-19 in 27 Countries. PLoS One. 2020;15(7):e0235590. doi:10.1371/journal.pone.0235590
18. Liu K, Chen Y, Lin R, Han K. Clinical features of COVID-19 in elderly patients: a comparison with young and middle-aged patients. J Infect. 2020;80(6):e14–e18. doi:10.1016/j.jinf.2020.03.005
19. Riad A, Jouzová A, Üstün B, et al. COVID-19 vaccine acceptance of pregnant and lactating women (PLW) in Czechia: an analytical cross-sectional study. Int J Environ Res. 2021;18(24):13373. doi:10.3390/ijerph182413373
20. Allotey J, Stallings E, Bonet M, et al. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: living systematic review and meta-analysis. BMJ. 2020;370:m3320. doi:10.1136/bmj.m3320
21. Antoun L, Taweel NE, Ahmed I, Patni S, Honest H. Maternal COVID-19 infection, clinical characteristics, pregnancy, and neonatal outcome: a prospective cohort study. Eur J Obstet Gynecol Reprod Biol. 2020;252:559–562. doi:10.1016/j.ejogrb.2020.07.008
22. Saccone G, Florio A, Aiello F, et al. Psychological impact of coronavirus disease 2019 in pregnant women. Am J Obstet Gynecol. 2020;223(2):293–295. doi:10.1016/j.ajog.2020.05.003
23. Schaal NK, Marca-Ghaemmaghami P, Preis H, Mahaffey B, Lobel M, Amiel Castro R. The German version of the pandemic-related pregnancy stress scale: a validation study. Eur J Obstet Gynecol Reprod Biol. 2021;256:40–45. doi:10.1016/j.ejogrb.2020.10.062
24. Preis H, Mahaffey B, Heiselman C, Lobel M. Pandemic-related pregnancy stress and anxiety among women pregnant during the coronavirus disease 2019 pandemic. Am J Obstet Gynecol MFM. 2020;2(3):100155. doi:10.1016/j.ajogmf.2020.100155
25. Jering KS, Claggett BL, Cunningham JW, et al. Clinical characteristics and outcomes of hospitalized women giving birth with and without COVID-19. JAMA Intern Med. 2021;181(5):714–717. doi:10.1001/jamainternmed.2020.9241
26. Villar J, Ariff S, Gunier RB, et al. Maternal and neonatal morbidity and mortality among pregnant women with and without COVID-19 infection: the INTERCOVID multinational cohort. JAMA Pediatr. 2021;175(8):817–826. doi:10.1001/jamapediatrics.2021.1050
27. Sutton D, D’Alton M, Zhang Y, et al. COVID-19 vaccine acceptance among pregnant, breastfeeding, and nonpregnant reproductive-aged women. Am J Obstet Gynecol. 2021;3(5):100403. doi:10.1016/j.ajogmf.2021.100403
28. Individuals using the Internet (% of population)–Saudi Arabia Data. Available from: data.worldbank.org/indicator/IT.NET.USER.ZS?locations=SA.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.