")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Training Medical Student Counselors for the Rochester Model, a Hospital Tobacco Treatment Program
Authors Grable JC , Shan K , Wang M, Han DD , Sportiello K , Chang M , Sysol JR, Bugbee D, Peltzer K
Received 5 November 2023
Accepted for publication 15 January 2024
Published 7 February 2024 Volume 2024:17 Pages 601—607
DOI https://doi.org/10.2147/JMDH.S447462
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
John C Grable,1,* Kevin Shan,1,* Matthew Wang,1,* Daniel D Han,1,* Kristen Sportiello,1,* Melissa Chang,1,* Justin R Sysol,1,* Doris Bugbee,2,* Kenneth Peltzer1,*
1Department of Medicine, University of Rochester School of Medicine, Rochester, NY, USA; 2Department of Nursing, University of Rochester School of Medicine, Rochester, NY, USA
*These authors contributed equally to this work
Correspondence: John C Grable, University of Rochester School of Medicine, 601 Elmwood Avenue, Rochester, NY, 14642, USA, Tel +1 585-275-7424, Fax +1 585-276-2820, Email [email protected]
Purpose: Providing effective tobacco dependence treatments to hospitalized patients remains a challenge. Prior to 2021, the Rochester Model program used staff nurses for both bedside and post-discharge counseling necessary to maintain abstinence. When nurse shortages and elevated job stress occurred during the COVID Pandemic, we proposed that medical students learn to counsel patients at the bedside and after discharge.
Patients and Methods: Due to COVID restrictions, first- and second-year medical students trained using remote Zoom sessions. The total training time was 2.5 hr without role-play or additional evaluations. A survey measured the students’ satisfaction, confidence, and counseling barriers. A smoking patient on a participating hospital unit can enroll in the program. Students delivered bedside counseling, then provided follow-up treatment and outcome calls along with New York State Quitline counselors.
Results: The survey demonstrated that 89% of the students were satisfied with the training. The bedside counseling confidence was greater than the phone counseling confidence. All students felt the program experience has value to them as future physicians. 124 smoking patients enrolled, and outcomes followed out to 6 months. The 7-day point prevalence quit rates using the as-treated (patients contacted) analysis were 57% at 4 weeks, 48% at 3 months, and 43% at 6 months. The 7-day point prevalence quit rates using the intent-to-treat (all patients) analysis were 31% at 4 weeks, 16% at 3 months and 14% at 6 months.
Conclusion: Medical students given minimal training are effective tobacco cessation counselors at no cost to the hospital system. The Rochester Model program using student counseling benefits patients, the students, and the health-care system.
Plain Language Summary: Hospitalization is an opportunity to help smokers quit. Successful programs require both bedside counseling and post-discharge contacts beyond a month. Cost remains the major issue for treating hospitalized smokers. Prior to the COVID Pandemic, the Rochester Model program used hospital nurses as bedside, post-discharge call counselors and champions. However, during the Pandemic, nurse shortages and work stress reduced their participation. Medical students seeking early patient contact trained as counselors, and the program shows promising quit rates at no cost. The Rochester Model supports the real-world application of medical students in hospital tobacco treatment programs.
Keywords: tobacco dependence treatment, medical students, nurse counseling, quit-line counseling
Introduction
A hospital admission is a “window of opportunity” to assist smoking patients in a quit attempt.1,2
Evidence shows that inpatient tobacco treatment increases cessation rates,3 decreases readmissions,4 and lowers costs.5 Major obstacles include the cost of a specialist counselor or the barriers of training staff to counsel.6 Tobacco treatment specialists (TTS) and specialist respiratory therapists can serve as bedside counselors when institutional or grant support is available.5,7 Furthermore, long-term abstinence requires patient contacts beyond a month after discharge.1 Phone calls after discharge are difficult for hospitals to implement due to lack of personnel, time, and support.6 Interactive Voice Response (IVR) systems are available for post-discharge calls with considerable costs.5,7 Funding comprehensive hospital tobacco programs remains a significant issue for hospital systems.
Medical students are a potential resource for counseling hospitalized smoking patients. Previous studies show that trained students can perform both outpatient and inpatient tobacco cessation counseling. Given multimodal education, students engaged in more smoking counseling behaviors than a control group in an outpatient setting.8 While teaching modules improved medical student counseling behaviors,9 it was found that role-play and direct patient interaction were the most efficient tools.10 A trial showed that hospitalized smokers given student counseling with a single post-discharge contact showed improvements in quitting motivation, pharmacotherapy use, and abstinence.11 A recent randomized controlled trial trained medical students to provide an inpatient counseling session and three post-discharge contacts. The six months, 7-day quit rate for the intervention group was 54.8% compared to 42% for the control group.12,13
The Rochester Model tobacco treatment program used nurse delivered bedside counseling followed by post-discharge calls by the New York State (NYS) Quitline and University of Rochester (UR) counselors.14 In 2021, during the COVID Pandemic, nursing staff shortages and work stress caused a reduction in nurse participation. In response, medical students were trained to counsel smoking patients at their bedside and post discharge. This report describes the training sessions, the students’ evaluation of the training and the preliminary program results.
Materials and Methods
Design, Setting, and Population
The Rochester Model (RM) program started in 2014.14 This project was undertaken as a QI initiative, and as per the University of Rochester’s Guideline for Determining Human Subject Research it did not meet the definition of research according to 45CFR46 and does not require IRB review. Medicine and Nursing administrators approved this QI project to be systematically implemented. Strong Memorial Hospital (SMH) has 886 beds with 39,000 annual admissions in Rochester, NY. Medical students counseled patients on units 714, 614, 634, 536, 516, 416, and 436. These units represent three medicine, two neurology, and two cardiac units. Active smokers of any amount admitted to a participating unit could enroll.
Screening and Enrollment
A unit clerk (tracker) screens admissions for smoking (Figure 1). An enroller (JG or JS) briefly explains the program to smoking patients. The enroller gives outpatient resources if the patient declines to enroll. When a patient joins, the enroller emails the student program coordinator to give the patient’s name and bed location.
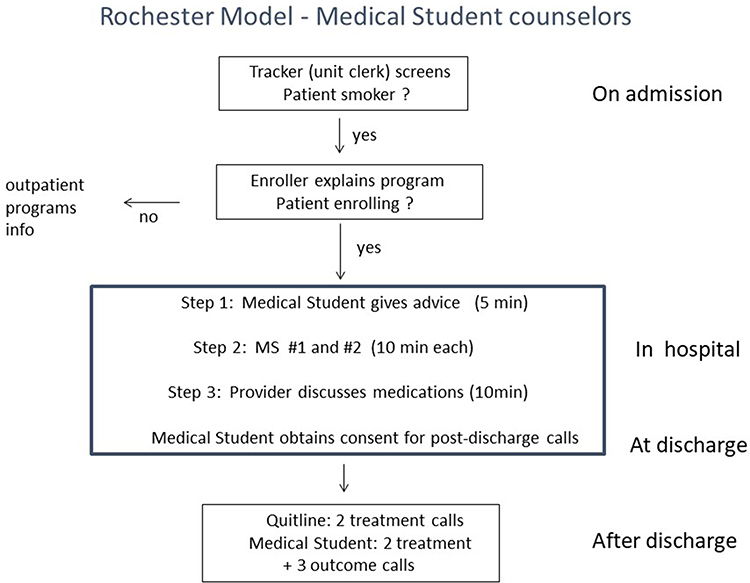 |
Figure 1 Rochester Model protocol. Step 1, Step 2, and Step 3 follow early in the hospitalization. Then the student obtains signed patient consent for the post-discharge calls. The enroller (JG) places the e-referral to the NYS Quitline upon discharge. |
Medical Student Volunteers at the University of Rochester
Most medical students have exposure to patients during third- and fourth-year rotations. First and second year medical students seeking early patient contact can earn a distinction in Community Health or nomination to the Gold Humanism Society by volunteering for this program. Students need to record 40 hr for the first and second years, 30 hr for third and fourth years to fulfill the requirement for this distinction.
Role of Medical Student Program Coordinator and Student Recruitment
Each year, 1–2 students volunteered to serve as coordinators. The coordinator recruits incoming medical students, schedules training sessions, and assigns patients to student counselors. The coordinators initiated an organization so that students receive credit for their counseling time. Coordinators recruited during an activity fair held each September and sent recruitment emails after 3 weeks. Recruitment emails were repeated in January and June to ensure that the program maintains an adequate number of counselors throughout the year.
Training of Medical Students for Bedside Counseling
From 1/22/22-6/1/23, a total of 29 first- and second-year students trained in smoking counseling. Due to Pandemic restrictions, a trainer (JG) held remote training sessions using Zoom. The training involved 5–10 students per session and lasted about 60 min. The trainer (JG) presented the clinical protocol (Figure 1) highlighting the students’ roles. The trainer used segments from the “Clearing the Air” manual15 to outline bedside counseling (MS #1 and MS #2). Essential elements include the patient’s motivation to quit, secondhand smoke, a nicotine addiction scale, smoking triggers, coping skills, and obtaining social support. The trainer then reviews a referral form for post discharge calls. The session content was similar for each group of students. Three medical students elected to leave the program.
Training of Medical Students for Post-Discharge Call Counseling
A week later, the trainer (JG) held a second remote session for post-discharge counseling.
The students review a teaching module developed by a fourth-year medical student. This module reviews cessation benefits, the program steps, and phone counseling strategies. Then, a 60-min Zoom session reviews the calling schedule, counseling tactics, and reinforcement of the hospital quit plan. The session outlines the collection of demographic data, smoking information, and tips for reaching patients. The teaching session did not include role-play.
Survey of Training, Confidence Levels, and Barriers
The trainer sent out a confidential survey a month after training to determine the students’ prior counseling experience, to assess training, confidence levels, and counseling barriers. Twenty-six of the medical students responded, as shown in Table 1.
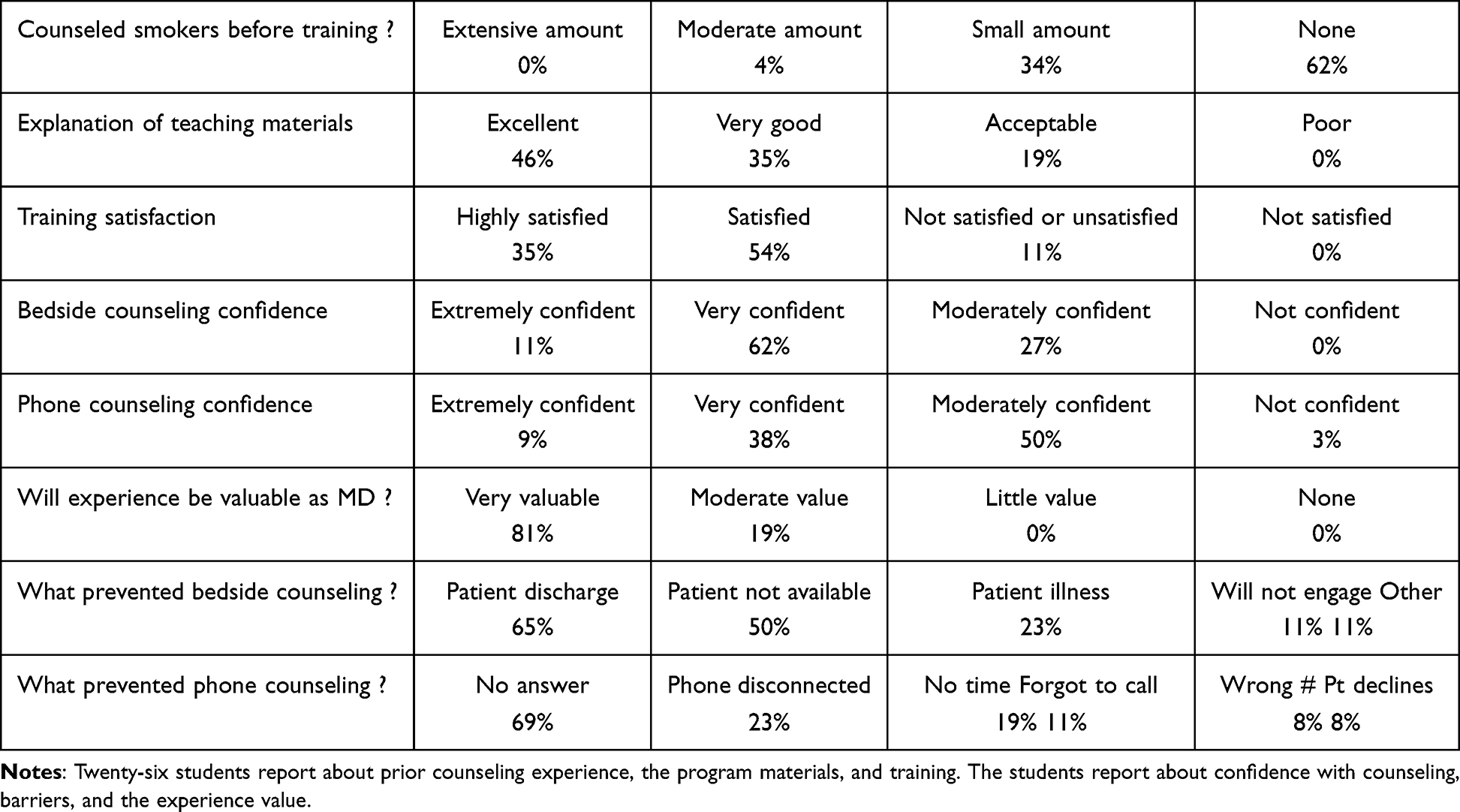 |
Table 1 Medical Student Survey |
Program Costs
There is no cost to the University of Rochester to operate the program. In comparison, a Tobacco Treatment Service using a TTS counselor with an IVR system reports yearly costs of $143,000.5
Inpatient Intervention
The enroller (JG or JS) briefly describes the program to hospitalized smokers (Figure 1). When a patient agrees, the enroller emails the coordinators to assign a counselor. As the patient’s condition dictates, the student counselor gives advice to stop smoking (Step 1). Then, the student gives MS #1, using “Clearing the Air” segments to discuss motivation, secondhand smoke, and nicotine addiction (Step 2). After this, the student gives MS #2, discussing triggers, coping behaviors, and completes a summary worksheet. Both counseling sessions together require approximately 30 min. Pharmacotherapy is the standard of care for inpatient smokers,16 so the student notifies the hospital providers to discuss nicotine replacement, Bupropion or Chantix (Step 3). The student then obtains a signed consent form from the patient to update contact information and give permission for the calls. On discharge, hospital providers prescribe appropriate pharmacotherapy to the patient. Student counselors do not follow patients discharged before the counseling steps.
Treatment and Outcome Calls and Evaluation Methods
The program provides four treatment calls as four calls are effective to maintain abstinence.17 Patients are first e-referred to the NYS quit line for two treatment calls within 2 weeks. Then, the student conducts two treatment calls (3-and 6 weeks) and three outcome calls (4 weeks, 3-and 6 months) to that patient. The treatment calls review progress with smoking triggers, relapses, cravings, and social support in 15–20 min. The outcome calls determine if patients smoked at all (self-report) in the last 7 days defining the 7-day point prevalence.18 Counselors attempt five treatment or outcome calls at the appropriate time point. A designation of “not reached” applies to patients when counselors could not make contact at two successive time points (a total of 10 attempts). The designation “smoker” applies to patients who decline calls or request to stop the calls. Counselors collect demographic and smoking data shown in Table 2 during an initial call.
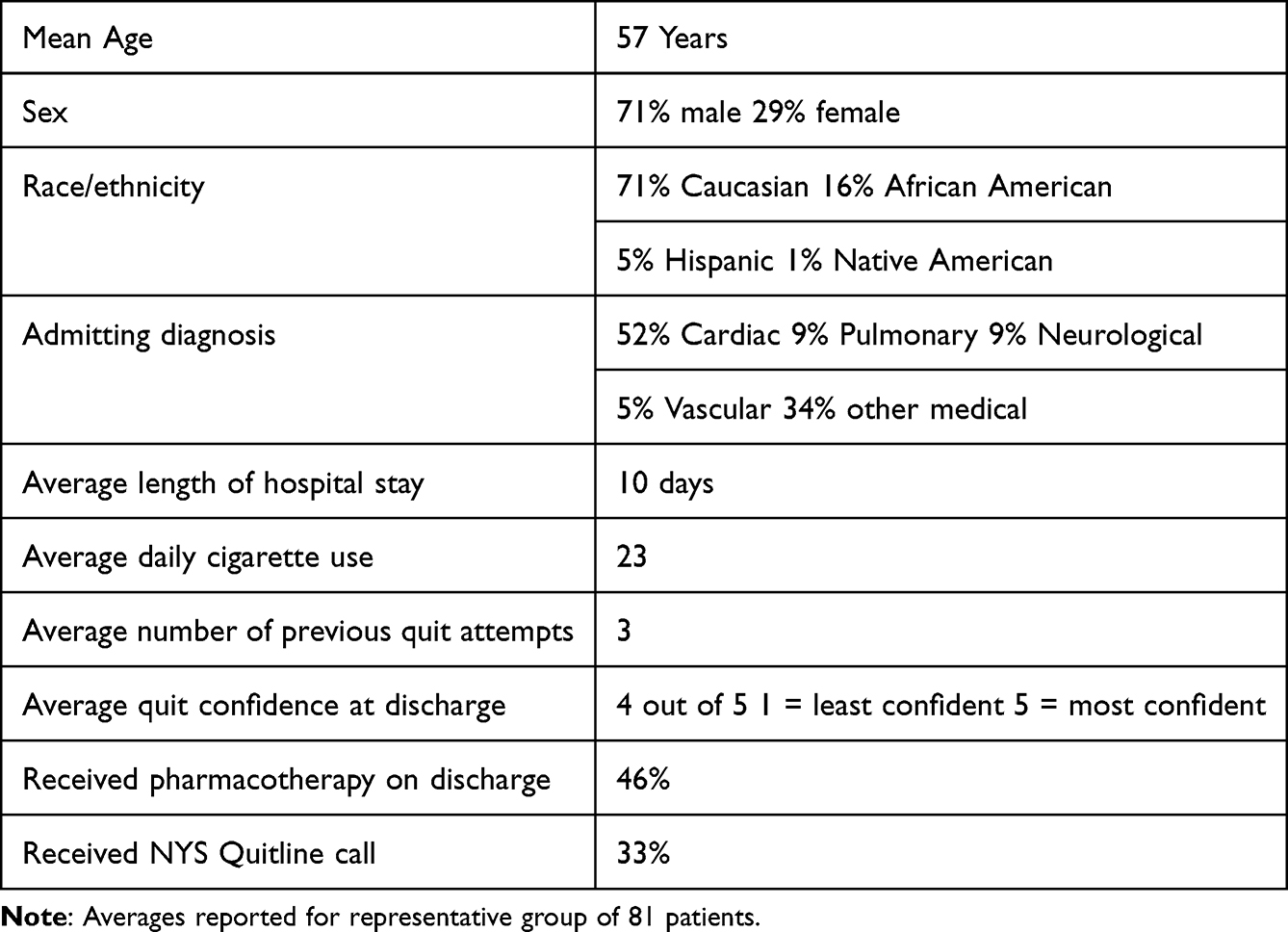 |
Table 2 Demographic and Smoking Data on 81 Patients from 1/29/22 to 7/24/23 |
Data Analysis
Self-reported 7-day point prevalence abstinence at 4 weeks, 3-and 6 months determine the quit rates. Reported are the quit rates using the as-treated (AT) analysis and the intention-to-treat (ITT) analysis. The AT analysis includes patients contacted by phone. For the AT analysis, the quit rate = number of patients quit/number of patients contacted (quit + smokers). The ITT analysis includes all patients if contacted or lost to follow-up. For the ITT analysis, the quit rate = number of patients quit/number of all patients (quit+ smokers + not reached) at a time point. A log-binomial model with a random intercept estimates the 95% CI.
Results
Screening and Enrollment Data
The program screened 451 smoking patients with 124 patients followed to 6 months from 1/29/22 to 7/24/23.
Demographic and Smoking Data
Eighty-one patients reported demographic and smoking data shown in Table 2. This group had 52% cardiac diagnoses, an average quit confidence of 80% and 46% received pharmacotherapy after discharge.
Medical Student Survey Data
Table 1 shows the confidential responses of 26 student counselors. Prior to training, 62% of students had no experience counseling smokers. The students rated the training materials explanation as acceptable to excellent, and 89% were satisfied with the training. Student confidence in bedside counseling was higher than phone counseling confidence. All students anticipate the program experience will be valuable to them as future physicians. The common barriers to bedside counseling were patient discharge, availability, and illness. The common barriers to phone counseling were patients not answering or a disconnected phone.
Smoking Cessation Outcome Data
The program enrolled 124 patients and followed them through 6 months from 1/29/22 to 7/24/23.
Using AT analysis (patients contacted) the 7-day point prevalence quit rates at 4 weeks, 3-and 6 months are 57% (39/68), 48% (20/42), and 45% (18/40), respectively. Using the ITT analysis (all patients) the 7-day point prevalence quit rates at 4 weeks, 3-and 6 months are 32% (39/124), 16% (20/124), and 15% (18/124), respectively (Figure 2). This data compares favorably to the previous RM cessation data.14 For that AT analysis, the 7-day point prevalence quit rates at 4 weeks, 3-and 6 months were 50% (89/178), 42% (63/151), and 38% (54/143), respectively. Using the ITT analysis (all patients) the 7-day point prevalence quit rates at 4 weeks, 3-and 6 months were 23% (89/385), 16% (63/385), and 14% (54/385), respectively. A sample of 20 patients who declined the program showed a quit rate of 20% at 4 weeks using AT analysis.14
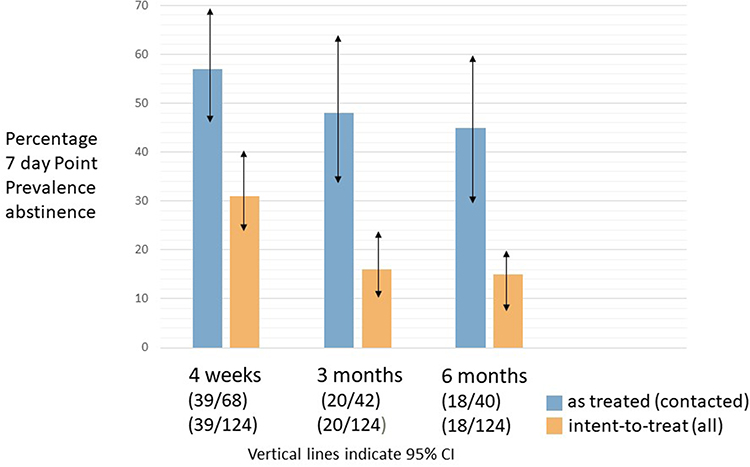 |
Figure 2 Rochester Model program percentage of 7-day point prevalence abstinence. Blue bars represent the as-treated (patients contacted) analysis, Orange bars indicate the intent-to-treat analysis (all patients) at each time point. Displayed are 95% Confidence intervals. |
Discussion
Prior to 2021, the program utilized staff nurses as bedside counselors, post-discharge call counselors, and champions.14 During the Pandemic, personnel shortages, and work stress caused a reduction in nurse counseling. In January 2022, medical students assumed the roles of bedside counselors, call counselors, and program coordinators.
The student training provided for the program is brief and performed remotely without additional evaluations. Training times from previous reports ranged from 4 hours plus role-play8,9 to an entire day.11 The most recent MSCHAT trial12,13 used three lecture hours, two role-play hours, booster sessions, and evaluations for second-year students. The Rochester Model trained first- and second-year students remotely due to COVID restrictions in 2 hr and 30 min without role-play or evaluations. Despite the abbreviated time and remote sessions, students reported satisfaction with the explanations and the training. The bedside counseling confidence was higher than the phone counseling while all students felt the experience was valuable. Students gain early patient contact, continuity of care, and receive credit from this program. Preliminary data of the 6-month quit rate exceed a benchmark self-report AT quit rate of 25% for hospital programs.17 Future directions for this program include adding a text messaging system to post-discharge contacts and replicating the program at another medical center.
Limitations
The program needs evaluation using implementation processes.19 The program requires assessments of student knowledge and counseling proficiency.9–11 Limitations of this report include incomplete demographic/smoking data and lack of biochemical verification.
Conclusions
Using medical student counselors, the Rochester Model program is showing promising quit rates and fulfilling Joint Commission guidelines for treatment of inpatient smokers.16 Medical students trained using brief sessions treated hospitalized smokers at no cost. The Rochester Model program with student counseling benefits patients, students, and health-care system.
Acknowledgments
The authors acknowledge the participation of all University of Rochester medical students who served as counselors for this program.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Rigotti NA, Clair C, Munafo MR, Stead LF. Interventions for smoking cessation in Hospitalized patients. Cochrane Database Syst Rev. 2012;5(5):CD001837. doi:10.1002/14651858.CD001837.pub3
2. Rigotti NA, Stoney C. CHARTing the Future Course of Tobacco-Cessation Interventions for Hospitalized Smokers. Am J Prev Med. 2016;51:549–550. doi:10.1016/j.amepre.2016.07.012
3. Trapskin PJ, Sheehy A, Creswell PD, et al. Development of a Pharmacist-Led Opt-Out Cessation Treatment Protocol for Combustible Tobacco Smoking Within Inpatient Settings. Hospital Pharmacy. 2021:I–9. doi:10.1177/001857821999809
4. Cartmell KB, Dooley M, Muller M, et al. Effect of an Evidence-based Inpatient Tobacco Dependence Treatment Service on 30-,90-and 180-day Hospital Readmission Rates. Med Care. 2018;56(4):358–363. doi:10.1097/MLR.0000000000000884
5. Cartmell KB, Dismuke CE, Dooley M, et al. Effect of an Evidence-based Inpatient Tobacco Dependence Treatment Service on 1-year Post discharge Health Care Costs. Med Care. 2018;56(10):883–889. doi:10.1097/MLR.0000000000000979
6. Sharpe T, Alsahlanee A, Ward K, Doyle F. Systematic review of Clinician-Reported Barriers to Provision of Smoking Cessation Interventions in Hospital Inpatient Settings. J Smoking Cessation. 2018;13(4):233–243. doi:10.1017/jsc.2017.25
7. Palmer AM, Rojewski AM, Chen LS, et al. Tobacco Treatment Program Model in US Hospitals and Outpatient Centers on Behalf of the SRNT Treatment Network. Chest. 2021;159(4):1652–1663. doi:10.1016/j.chest2020.11.025
8. Ockene JK, Hayes RB, Churchill LC, et al. Teaching Medical Students to Help Patient Quit Smoking: outcomes of a 10-School Randomized Controlled Trial. J Gen Internal Med. 2015;31(2):172–181. doi:10.1007/s11606-015-3508-y
9. Herold R, Schiekirka S, Brown J, et al. Structured Smoking Cessation Training for Medical Students: a prospective Study. Nicotine Tobacco Res. 2016;18(2):2209–2215. doi:10.1093/ntr/ntw191
10. Stolz D, Langewiitz W, Meyer A, et al. Enhanced Didactic Methods of Smoking Cessation Training for Medical Students- A Randomized Study. Nicotine Tobacco Res. 2012;14(2):224–228. doi:10.1093/ntr/ntr186
11. Kumar A, Ward K, Mellon L, et al. Medical Student Intervention to promote effective nicotine dependence and tobacco HEalthcare (MIND-THE-GAP): single-centre feasibility randomized trial results. BMC Med Educ. 2017;17:249. doi:10.1186/s12909-017-1069-y
12. Satish P, Khetan A, Shah D, et al. Rational and Design of a Randomized Trial to Evaluate the Effectiveness of Medical Student Counseling for Hospitalized Patients Addicted to Tobacco (the MS- CHAT Trial). J Smoking Cessation. 2021. doi:10.1155/2021/6682408
13. Satish P, Khetan A, Shah A, et al. Effectiveness of Medical Student Counseling for Hospitalized Patient Addicted to Tobacco (MS-CHAT): a Randomized Controlled Trial. J Gen Intern Med. 2023:1–9. doi:10.1007/s11606-023-08243-y
14. Grable J, Lin J, Peltzer K, et al. Integrating Tobacco Dependence Treatment into Hospital Practice Using the Rochester Model. J Multidisciplinary Healthcare. 2023;16:905–911. doi:10.2147/JMDH.S400615
15. National Cancer Institute. Clearing the Air. NIH Publication No. 08-1647; 2008.
16. Fiore MC, Goplerud E, Schroeder SA. The Joint Commission’s New Tobacco Cessation Measures-Will Hospitals Do the Right Thing? NEJM. 2012;366(13):1172–1174. doi:10.1056/NEJMp1115176
17. Taylor CB, Miller NH, Cameron R, Fagans EW, Das S. Dissemination of an effective inpatient tobacco use cessation program. Nicotine Tobacco Res. 2005;7(1):129–137. doi:10.1080/14622200412331328420
18. Cheung KL, De Ruijter D, Hiligsmann M, et al. Exploring Consensus on how to measure smoking cessation. A Delphi Study. BMC Public Health. 2017;17(890). doi:10.1186/s12889-017-4902-7
19. Pearson N, Naylor PJ, Ashe M, Fernandez M, Yoong SL, Wolfenden L. Guidance for conducting feasibility and pilot studies for implementation trials. BMC. 2020;6:167.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.